![]()

|
|
>
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com No texting or chat messages, please. Ordinary e-mails are welcome. Your confidentiality is completely respected.
I am active in HealthTap, which provides free medical guidance from your cell phone. There is also a fee site at www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 | With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with peoples' health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:

My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship by suspending their own reasoning and
simply accepting a single authority that seems wise and good. I've learned that they leave the movements when, and only when, they discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!

![]()
![]()
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
![]() How to work up
How to work up
a muscle biopsy
Oklahoma
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- Nerve / Muscle
Lectures follow Textbook
| QUIZBANK Muscle & soft tissue (all except #'s 55-61) |
INTRODUCTION
|
{14614} skeletal muscle, histology
{20723} skeletal muscle, histology {44101} skeletal muscle, ultrastructure {44116} mitochondrion & sliding filaments {44110} section of myofilaments {18639} {18643} {18644} {18665} |  |
You already know the basics:
Skeletal ("striated") muscle is for posture and locomotion. Its syncytial, multinucleate cells ("myocytes", "myofibers", "muscle fibers") may be as thick as 100 microns, and are as long as the muscle itself.
Fewer than 3-5% (usually much fewer) of nuclei should be centrally located, with the rest beneath the sarcolemma.
There is no need to review actin and myosin (the "myofilaments"), sarcomeres (the basic units laid end-to-end to form "myofibrils"), bands, endomysium (the connective tissue around a muscle cell), perimysium (the connective tissue around a group of fibers, or "fascicle"), or epimysium ("fascia").
By contrast, exactly how skeletal muscle gets bigger (from strength training) and smaller (from disuse or disease) remains mysterious (Lancet 357: 734, 2001).
* The signal molecule Notch seems to cause differentiation of muscle stem cells into myocytes (J. Cell. Phys. 208: 538, 2006). Myogenin is a regulatory molecule that seems to promote muscle growth after hard work / injury (Clin. Genet. 57: 16, 2000. Watch myostatin closely.
* In studies of older men being given exogenous testosterone (which by itself bulks the muscles and causes satellite cells to proliferate and differentiate into new muscle cells), intranuclear myogenin and activated Notch were greatly increased in the treament group (J. Clin. Endo. Metab. 91: 3024, 2006.)
One lower motor neuron and the (usually several) muscle cells that it innervates make up a motor unit.
Pathologists seldom pay much attention to non-fatal physical injuries involving muscle, tendon, or ligament.
SPRAINS are damaged ligaments. The pain is from the microbleeds and edema. Here's a grading system:
STRAINS result from physical stretching of muscle in opposite directions ("pulled muscle"). Capillaries and fibers are torn. They're most severe at the muscle-tendon junction (where the force is greatest; why?);
* Anecdotally, following torture on the rack, muscles stretched very long would be rendered permanently non-functional. Was this from separation of the sarcomere filaments, from nerve damage, or from tendon rupture? No one knows. Remember that torture for political repression or to obtain confessions that may or may not be true remains an ugly fact in much of the world, even today. More about this, and what physicians are doing to stop it, later.
Their ultrastructural correlates, which must be interesting, have not been well-studied.
Bruises (contusion) of muscle require no description. Although a study with histology shows faster healing if the bruises are immobilized (J. Bone Joint. Surg. 92: 894, 2010), this is unlikely to be popular with patients, who will recover regardless.
Nobody really understands the common CRAMPS -- involuntary, painful, sudden skeletal muscle contractions. Usually they follow a strong voluntary contraction, and as everyone knows, these can usually be stopped if the muscle can be stretched.
HEAT CRAMPS occur when blood volume and/or blood sodium are low because of sweating, in the muscles that have been exercised most heavily. The muscles are painful and contract on their own. They often occur after the exertion is over, especially when serum sodium remains low (i.e., you replaced your water but not your sodium.)
BLACK WIDOW SPIDER ENVENOMATION produces some of the most impressive cramps in medicine.
NOCTURNAL LEG CRAMPS have no known anatomic correlate. Anyone can get them, but especially older folks and women in late pregnancy. Try stretching before retiring, staying well-hydrated, getting enough magnesium in the diet (you think?), and perhaps taking quinine.
BENIGN FASCICULATION SYNDROME ("benign cramp fasciculations", etc.) is a poorly-understood, common non-disease in which muscles not in use get "the twitchies", especially the calves, especially when the person is tired. It doesn't progress. Everybody gets a few twitches now and then; nobody understands this either.
RESTLESS LEGS SYNDROME is a parasomnia rather than a muscle disease. By keeping you from getting restorative sleep, it can ruin your life. Update Am. Fam. Phys. 78: 235, 2008 (rule out iron deficiency, Rx's, pregnancy).
* Whiplash is probably strain-sprain of the neck from acceleration-deceleration, with perhaps some damage to the brainstem (PET scan J. Neur. Neurosurg. Psy. 63: 373, 1997; more J. Trauma 52: 521, 2002), with an overlay from the lawyers. When you could no longer get damages for pain and suffering, patients got much better much faster (NEJM 342: 1211, 2000). If you believe that it's fundamentally a spine problem, you'll have trouble explaining the negative results of injection therapy (NEJM 330: 1083, 1994).
Grade I-II strains and sprains get better in a few months at most, regardless. New radiologic techniques have clarified what happens in the vertebrae: the ventral lesions result from overstretching ("tensile failure") of the joint capsule, and the dorsal lesions from pinching the joint capsule / synovium as the facets are smashed together (Spine 29: 1764, 2004). If something else is happening to the brainstem, imaging has not revealed it.
Muscle fibers are divided into two histochemical types:
Slow-twitch ("red fibers", "type I fibers", "myoglobin-, bulky sacromere-, lipid- and mitochondrion-rich", "oxidative muscle", "dark meat", "marathon muscle", "one slow red ox") are responsible for maintaining posture and help with both strength and endurance athletics.
Fast-twitch ("white fibers", "type II fibers", "glycogen-rich", "glycolytic enzyme-rich", "glycolytic muscle", "white meat", "sprinter muscle"; ATP-ase-rich muscle) are responsible for rapid contraction and bursts of speed.
The fiber type is determined by the axon that currently supplies it. Some lower motor neurons innervate type I fibers, while others innervate type II fibers. Since there are so many neurons, the arrangement of type I and type II fibers should seem random in health.
{14381} normal; NADH stain with type I fibers dark, type II fibers light
{14418} normal; ATPase stain with type I
fibers dark, type II fibers light
Unlike in chickens, each of our named muscles contains a mix of these two fiber types. Within broad guidelines (i.e., postural muscles like soleus are mostly slow-twitch), your genes determine the relative proportions of type I and type II fibers in individual muscles. Communist-bloc coaches used to biopsy their prospective olympians to help them match sports to muscle fiber type predominance.
Diseases that involve primarily the muscle cells typically present as weakness (look for a baby's head flopping, a child's exaggerated lumbar lordosis, or in an older person, bow legs, difficulty getting out of a chair, winging of the scapula), and maybe atrophy.
Myotonia is characteristic of a few muscle problems; it may be "grip myotonia" (i.e., the muscles remain contracted for too long after they are used), and/or "percussion myotonia" (i.e., the muscles contract when handled). Myotonic dystrophy people usually have both. The problem, of course, is repetitive electrical activity on the sarcolemma.
While the pattern of muscle involvement may suggest a diagnosis, often muscle biopsy is required. Sore muscles are more likely to be due to vasculitis (lupus, polyarteritis nodosa), strain, infections (remember trichinosis), rhabdomyolysis, or polymyositis.
|
|
|
| REACTIONS OF MUSCLE CELLS Simple atrophy of muscle cells occurs when they are (1) deprived of its nerve supply ("neurogenic atrophy"), or (2) deprived of its blood supply ("ischemic atrophy"), or (3) not used ("disuse atrophy") or, (4) subjected to glucocorticoids (today, that's mostly "iatrogenic atrophy"). * (5) vitamin D deficient (more common than you think? Arch. Int. Med. 160: 1199, 2000; update on the epidemic of vitamin D deficiency in young American women and its link to increased fat overall and specifically within muscle: J. Clin. Endo. Metab. 95: 1595, 2010; same finding on imaging in the vitamin D-deficient elderly AJR 194: 728, 2010) |  |
Disuse atrophy and glucocorticoid atrophy involve primarily type II fibers.
![]() type II muscle atrophy
type II muscle atrophy
Wash. U., St. Louis
Illustrated notes
{14430} disuse or glucocorticoid atrophy, type II fibers
Degeneration of muscle fibers usually means "focal coagulation necrosis", or something very much like it.
Fibers shrivel, lose good cross-striations, become hypereosinophilic ("Zenker's hyaline change"), exhibit local nuclear pyknosis, and get entered and eaten by visiting macrophages. (Rule: Macrophages eating dead muscle do not indicate inflammation. A significant number of lymphocytes or neutrophils does indicate inflammation.)
Degeneration is typically segmental. The fiber can regenerate itself as long as the endomysial tubule is intact.
{14414} degenerating fibers, early Duchenne's
|
|
Regeneration of muscle fibers is a common finding.
Reserve cells ("satellite cells"; nice pictures in Anat. Rec. 222: 6, 1988) in the endomysium proliferate as myoblasts, until the tube is re-filled. The fiber then regenerates.
Of course, regenerating fibers have basophilic cytoplasm, and centrally-located nuclei with lots of euchromatin and obvious nucleoli (i.e., they're busy).
* The genetic control of transformation of satellite cell to myoblast to myocyte is by now partly understood (Clin. Nutr. 9: 214, 2006). In fatal muscular dystrophy, current thinking is that death occurs when there are no longer any satellite cells to replace the fibers that die off.
Creatine seems to work its magic for bodybuilders by increasing the number of satellite cells, and their tendency to differentiate / donate nuclei to myocytes (J. Phys. 573: 525, 2006; Med. Sci. Sport. 35: 769, 2003). It also seems to increase strength even in kids with Duchenne's (Neurology 62: 1771, 2004). This suggests to me that the pop wisdom that creatine bulks muscle primarily by bringing in water isn't the full story.
Increased fiber size variation is a nonspecific finding, and may be seen in most muscle diseases, in prolonged neuropathic disease, or in any cause of type II fiber atrophy.
Increased numbers of central nuclei is nonspecific but indicates muscle fiber disease.
* Hypercontraction is hypereosinophilia of segments of fibers, where the sarcomeres are clamped shut. This is common in severe muscular dystrophy (i.e., Duchenne's). It's not clear how this differs from degeneration / necrosis (if it always does). Sometimes it is an artifact, i.e., you see it (with no surrounding tissue reaction) in muscle that's obtained without using a isometric clamp to keep the fibers from contracting on their own.
Target fibers: curious fibers with centrally-located masses of scrambled muscle filaments without mitochondria, lots of mitochondria and few sarcomeres in their intermediate areas, and normal sarcoplasm under their sarcolemmal membranes. When you see a target fiber, it almost always means denervation-reinnervation.
 Chronic partial denervation
Chronic partial denervation
Wash. U., St. Louis
Illustrated notes
{14393} several target fibers
Angular fibers are individual atrophic fibers or small groups of atrophic fibers; they are typically compressed by surrounding larger fibers. As noted above, think of any process that makes one fiber smaller than others (denervation is most typical, but anything that makes some fibers smaller than their neighbors can make them angular).
{14421} several angular fibers
![]() Neurogenic atrophy
Neurogenic atrophy
Tom Demark's Site
NOTE: Markedly variable sizes among neighboring fibers, without angularity or grouping, is more suggestive of muscular dystrophy.
NOTE: A cluster of atrophic cells, all of one type? Neurogenic atrophy (why?)
Ring fibers exhibit peripheral myofilaments that run circumferentially (* really spirals). While not specific (they may be an artifact of over-contraction), think of myotonic dystrophy.
 Split fibers is a misnomer. Fibers are clefted, with nuclei along the cleft. What has probably happened is either that (1) some regenerating myoblasts have not fused, or (2) we have had longitudinal division of a muscle cell to make
two. That was supposed to be impossible, but ask Arnold Schwarzenegger....
Split fibers is a misnomer. Fibers are clefted, with nuclei along the cleft. What has probably happened is either that (1) some regenerating myoblasts have not fused, or (2) we have had longitudinal division of a muscle cell to make
two. That was supposed to be impossible, but ask Arnold Schwarzenegger....
{25526} split fiber in early muscular dystrophy
Fibrosis (endomysium, perimysium) often follows inflammation and/or atrophy. Fatty ingrowth ("fatty infiltration", not to be confused with "fatty change") is often common in end-stage muscle. With a few exceptions, neither change is very helpful diagnostically.
Future clinicians: When doing a muscle biopsy, remember:
(1) Muscle biopsies hurt. Don't do muscle biopsies for "academic" curiosity. If you decide to do the biopsy, warn your patient.
(2) A muscle biopsy in Duchenne's will result in fibrosis and contracture of the muscle; suspected Duchenne's is a relative contraindication to the procedure.
(3) Select a muscle that is mildly, but definitely, involved. The pathology will show best here. (If a muscle isn't weak, the histology won't be abnormal. If the muscle is mostly fibrous tissue and fat, giving a specific diagnosis is probably impossible.
* (4) Don't biopsy near a tendon, or the pathologist may not know how to interpret the "fibrosis", uneven fiber size, and increased nuclei.
(5) Don't biopsy recent sites of injections or electromyography needle insertions.
* (6) The deltoid has an unusual connective tissue pattern, so let the pathologist know if this is your biopsy site.
(7) Keep the muscle fragment from contracting after biopsy. We'll give you a clamp.
(8) Today, the diagnosis of each of the common genetic muscle diseases is made on immunohistochemistry, usually on frozen sections, though with newer antibodies, paraffin-embedded tissue can be used (J. Clin. Path. 54: 517, 2001; fiber typing J. Clin. Path. 55: 375, 2002).
(9) Send us the specimen fresh; don't put it in formalin.
(10) If you suspect an inflammatory myopathy other than inclusion body myositis, consider taking two biopsies because of disease variability from place to place (Am. J. Clin. Path. 126: 843, 2006).
MYASTHENIA GRAVIS
In this disease, which is fairly common especially among young women, polyclonal antibodies attack (usually) the acetylcholine receptor (* bungarotoxin binding site) of the post-synaptic membrane of the neuromuscular junction. This causes weakness, since binding of acetylcholine is blocked, and receptors are degraded too rapidly.
Occasional patients lack autoantibodies against the acetyl-choline receptor; these people usually have antibodies against muscle-specific kinase (anti-MuSK) instead, and do not benefit from thymectomy (Brain 126: 2304, 2003; pathology of the animal model Neurology 69: 453, 2012) but may do well on rituximab (anti-B-cell treatment, Neurology 78: 189, 2012). Patients with anti-MUSK are much less likely to remit serologically / clinically (Neurology 80: 188, 2013.
Patients suffer from weakness, and tire easily. The disease usually begins in the eyes (droopy "ptotic" eyelids, double vision). You'll learn about the "Tensilon test" on rotations, though it seems to be going out of fashion. Like most autoimmune diseases, myasthenia gravis is a disease of exacerbations and remissions, and thanks to the "ICU", today's patients usually die of something else.
This is not an anatomic pathologist's disease. In a minority of patients clusters of lymphocytes (* "lymphorrhages") appear around the motor end plates (Arch. Path. Lab. Med. 112: 934, 1988; Neurology 41: 1497, 1991; Neurology 38: 1173, 1988).
Probably the ability to get myasthenia gravis is polygenic.
Interestingly, about 30% of these patients have a thymoma, and most of the rest have thymic hyperplasia (i.e., prominent germinal follicles in the thymus gland). Even if the thymus is atrophic like most other adults', it's best to come out (Ann. Thorac. Surg. 91: 212, 2011).
Most thymomas express acetylcholine receptor epitopes on the surfaces of the neoplastic cells (Lancet 339: 707, 1992; Am. J. Path. 148: 1359 & 1839, 1996). We can suppose for now that this is what triggers the disease.
Most people with myasthenia gravis who do not have antibodies against acetylcholine will have them against the receptor tyrosine kinase "muscle-specific kinase" (Nat. Med. 3: 365, 2001.
* Several other anti-muscle autoantibodies (anti-titin, anti-ryanodine-receptor; formerly "anti-striational antibodies") also commonly turn up in these people (Muscle & Nerve 21: 329, 1998; Arch. Neuro. 62: 442, 2005). Again, it's supposed to be molecular mimicry. "Thymomatous MG" and "MG with titin antibodies" now are considered separate entities: Arch. Neuro. 64: 1729, 2007).
* The thymoma may be too small to see on scan: Chest 131: 847, 2007 ("microthymoma").
Extended thymectomy (i.e., be sure you get the little bits of thymus a few cm away from where the gland is supposed to be located) seems to be the procedure of choice nowadays (Ann. Thoracic Surg. 62: 853, 1996). Some institutions are now doing thymectomies without sternotomy using special instruments (Am. J. Surg. 199: 589, 2010); "robotic thymectomy" Ann. Thorac. Surg. 92: 1018, 2011; J. Thorac. Card. Surg. 141: 673, 2011.
As with other autoimmune diseases, patients often have a second serious autoimmune disease. Look for Hashimoto's, lupus, rheumatoid arthritis, autoimmune thyroid disease.
* Of course the antibody can cross the placenta, and weaken the unborn child.
* The myasthenia organizations say that the dwarf "Sleepy" was modeled on one of Walt Disney's friends who had myasthenia gravis and droopy eyelids. Be this as it may, the dwarf is a mascot for people with the disease.
Other myasthenic syndromes: In addition to some genetic NMJ problems (Arch. Neuro. 56: 163, 1999), you need to remember the EATON-LAMBERT SYNDROME ("myasthenic myopathic syndrome"), a weakness syndrome typically seen with oat cell carcinoma of the lung, though sometimes alone. These patients make an autoantibody against calcium channels (NEJM 332: 1467, 1995 review) that blocks release of acetylcholine itself.
![]() Myasthenia gravis
Myasthenia gravis
Wash. U., St. Louis
Illustrated notes
|
MUSCLE CHANGES IN PERIPHERAL NERVE DISEASE
Denervation (i.e., lower motor neuron) changes in muscle occur only if the axon itself is damaged. (Contrast "demyelinating disease" of peripheral nerves, which leaves muscle unchanged.) Partially damaged nerve is the site of axonal sprouting, with axons from surviving neurons growing into the empty spaces once occupied by other axons. Since the current axon supplying a muscle cell determines whether it is a type I or a type II fiber, the redistribution of a diminished number of axons will result in type grouping of fibers, pathognomonic (in humans) of denervation-reinnervation. |
|
|
{14429} denervation-reinnervation pattern with type grouping; compare normal {14418} |
|
If the disease process continues, and the ability of axons to be replenished is reduced, look for group atrophy of muscle fibers. Sometimes you may see target fibers. Late in the disease, expect to see some myopathic changes, too.
{14353} neurogenic atrophy
Noteworthy causes of neurogenic atrophy include amyotrophic lateral sclerosis and a variety of other diseases. If denervation is rapid, muscle cells may twitch repetitively due to increased sensitization to acetylcholine, producing fasciculations.
WERDNIG-HOFFMAN DISEASE / INFANTILE SPINAL MUSCLE ATROPHY is an autosomal recessive disease of anterior horn cells causing them to die off, mostly before birth (Brain 125: 1624, 2002) and continuing through the child's short life. The genes are SMN ("survival motor neuron"). This produces extremely floppy babies, progressing to death in the first year (there are variants with longer survival). Histology shows atrophic groups of type I and type II fibers and occasional clusters of huge type I fibers. Other alleles produce other spinal muscle atrophy diseases; type II is "infantile-chronic".
{14372} Werdnig-Hoffman disease
{14375} Werdnig-Hoffman disease
{14403} Werdnig-Hoffman disease
![]() Spinal muscular atrophy
Spinal muscular atrophy
Wash U, St. Louis
* Sodium butyrate for SMA... well, it works in the knockout mouse (Proc. Nat. Acad. Sci. 98: 9808, 2001).
KUGELBERG-WELANDER DISEASE ("the mild counterpart of Werdnig-Hoffman", SMA III) is caused by another allele at the Werdnig-Hoffman locus. It is a milder disease defined to be seen in children who could once walk. All you'll see on muscle biopsy is type-grouping and atrophy. There is believed to be at least one even milder allele ("the adult form").
{14380} Kugelberg-Welander disease (note poor muscular development)
{14377} Kugelberg-Welander disease (Gower's sign like in
Duchenne's; see below)
CHARCOT-MARIE-TOOTH disease features neurogenic-type atrophy of the leg muscles, especially the calves ("champagne-bottle legs"). We'll talk about this under nerve diseases.
{14413} Charcot-Marie-Tooth disease, adult
{14407} Charcot-Marie-Tooth disease, kid
{14429} type grouping,
this was a case of Charcot- Marie-Tooth disease
In weakness caused by damage to the neurons in the cerebral cortex, of course, all you will see is widespread fiber atrophy, mostly of type II cells, from disuse. Since the muscle fibers are still innervated, they will not undergo real neurogenic atrophy.
MUSCULAR DYSTROPHY
This is a group of hereditary myopathies, considered together by custom. ("Dystrophy" is a traditional, basically meaningless word.) Short review Lancet 359: 687, 2002.
Common to these diseases is atrophy and loss of muscle fibers in the absence of nerve disease. Exactly how this happens is only now becoming clear, as the various proteins involved prove to form a membrane complex that gives strength and structure to the muscle cell.
Now is a good time to mention that, for a given locus, different mutations/alleles may give different syndromes. For example, a mutated gene for the calcium channel that is the receptor for ryanodine can produce limb-girdle dystrophy, malignant hyperthermia, central core disease, all-type-I-fiber disase without central cores, a dilated cardiomyopathy, or idiopathic cardiac rhythm problems (J. Clin. Inv. 115: 2033, 2005; especially sudden drowning Mayo Clin. Proc. 80: 596, 2005).
It's also a good time to mention that apparently healthy people with chronically elevated creatine kinase levels and who do not exercise usually have a "forme fruste" of one of the myopathies, with abnormal muscle biopsy (Neurology 66: 1585, 2006). Biopsy and/or gene-screeen if the patient is truly curious.
The kid who is "just not trying in gym class" may be singled out for abuse from teachers and peers for years before a muscle disease is found.
DUCHENNE'S MUSCULAR DYSTROPHY ("Jerry Lewis's kids")
This is a common (one male in 3500), sex-linked recessive trait. One third of cases are new mutations, and no population group is without these people. The fundamental lesion is a lack of dystrophin, an inner-sarcolemmal cytoskeletal component homologous to spectrin and actin, which appears to strengthen muscle cells and keep them from popping when overworked (Nature 349: 69 & 243, 1991; Proc. Nat. Acad. Sci. 90: 3710, 1993). The gene's on Xp21.
Although the children appear normal at birth, the muscle is already abnormal, and the problem becomes obvious in early childhood. These boys have symmetric weakness, and must resort to unusual methods to stand up ("Gower's sign"). Fatty ingrowth produces the characteristic "pseudohypertrophy of the calves". Boys become wheelchair-bound by their early teens.
About 1/3 of these boys are mentally retarded as a result of involvement of a portion of the locus that also involves a brain protein. Although results are conflicting, the allele seems to be the determining factor (Neurology 55: 559, 2000). Cardiomyopathy is also common (cardiomyopathy-only allele Circulation 87: 1854, 1993), and is a problem even for female carriers (JAMA 275: 1335, 1996 -- not a life-shortener, though Heart 94: 633, 2008).
The pathologist sees various myopathic changes, notably degeneration with phagocytosis and regeneration attempts along the muscle fibers. Even in muscles that are not yet weak, each fiber is usually ringed by fibrous tissue. As the necrosis predominates, the fibers are replaced by fat and scar tissue. The healthier fibers undergo hypertrophy, producing striking variability in the sizes of fibers. Myofiber types are poorly defined.
{14443} Duchenne's, kid
{14446} Duchenne's, kid
{14449} Duchenne's; Gower's sign
{14408} Duchenne's, early, dark-staining fibers are dying
{14411} Duchenne's, classic histopathology
{09036} Duchenne's, biopsy; trichrome stain (i.e., muscle red,
fibrosis blue)
![]() Duchenne muscular dystrophy
Duchenne muscular dystrophy
H&E
Wikimedia Commons
For some reason, affected boys and their carrier mothers have markedly elevated creatine kinase. Electron microscopists see breaks in the sarcolemma and the CK is probably leaking out here.
A woman carrying Duchenne's may be affected due to unfortunate lyonization (two with lyonization causing hemiatrophy: Arch. Neuro. 67: 497, 2010). By contrast, fortunate lyonization may produce a normal creatine kinase, obscuring the carrier state in the era before easy genetic screening. Of course, normally-lyonized carriers show immunostaining for dystrophin around about half of their myofibers (NEJM 321: 398, 1989). A Turner's woman or testicular-feminization "woman" can have the disease.
* Autosomal recessive syndromes indistinguishable clinically from Duchenne's are rare, but do occur (Am. J. Hum. Genet. 45: 63, 1989; Neurology 45: 768, 1995; Arch. Dis. Child. 64: 1501, 1989; adhalin deficiency J. Clin. Invest. 96: 1202, 1995.)
Gene therapy for Duchenne's has been a challenge because the molecule is so large (Nat. Med. 8: 253, 2002; Nat. Med. 9: 997, 2003); some trials are underway now, with injection of a vector into individual muscles (Arch. Neuro 64: 1236, 2007). Manipulating circulating stem cells works in mice: J. Clin. Inv. 114: 192, 2004. In one failure, dystrophin was not expressed but the immune system did become sensitized to it (NEJM 363: 1429, 2010).
* Myoblast transfer for Duchenne's, which works in an animal model, isn't working in people yet. For some reason, the myoblasts simply decide to die when introduced into the human body. NEJM 333: 838, 1995 was the last major review, but stay tuned.
* Creatine for Duchenne's: seems to help. Neurology 62: 1771, 2004. Antisense oligonucleotide shows promise: NEJM 364: 1513, 2011; trials are underway Hum. Gene Ther. 24: 479, 2013. MicroRNA-206 works in mice, stay tuned: J. Clin. Inv. 122: 2054, 2012.
Duchenne's patients have been maintained on respirators for as long as 30 years (Chest 123: 1307, 2003; don't do something like this to me).
* One's osteopontin (SPP1) allele affects the progression of Duchenne's (Neurology 76: 219, 2011).
BECKER'S MUSCULAR DYSTROPHY
"Another sex-linked muscular dystrophy", caused by milder abnormal alleles at the Duchenne's locus. "Becker's" is defined to be "Duchenne's" in which patients can still walk by their 16th birthday. It's less common than Duchenne's: Lancet 337: 1022, 1991; the cardiomyopathy Am. Heart J. 132: 642, 1996.
The problem in most cases is that dystrophin, though present, is mutated into a less-effective form. Dystrophin has several domains that do different things, and Becker's is very heterogeneous. For a recent review, see Brain 125: 4, 2002.
{14473} Becker's (I think; pseudohypertrophy of calves)
{14467} Becker's (I think; pseudohypertrophy)
{14470} Becker's (I think; pseudohypertrophy)
EMERY-DREIFUSS MUSCULAR DYSTROPHY is a comparatively mild disease cause by lack of a protein called "emerin" on the nuclear (rather than the sarcoplasmic) membrane (gene EMD on the X-chromosome Nat. Gen. 12: 252 & 264, 1996; a dominant locus at lamin A/C LMNA Brain 129: 996, 2006). The worst problem is the cardiomyopathy (why the heart: J. Clin. Inv. 117: 1282, 2007).
{27271} Emery-Dreifuss
{27274} Emery-Dreifuss
{27277} Emery-Dreifuss
{27280} Emery-Dreifuss
{27283} Emery-Dreifuss
{27352} Emery-Dreifuss
![]() Emery-Dreifuss
Emery-Dreifuss
Wash U, St. Louis
MYOTONIC DYSTROPHY (* "Steinert's disease")
This is an autosomal dominant (the most common locus cloned: gene DMPK -- "Steinert's" or "type I"; Science 255: 1253 & 1256, 1992; protein is "myotonin" Science 260: 235, 1993), variably expressed because of other genes, affecting several systems. In some communities, it is as common as Duchenne's.
Patients have:
{53755} myotonic dystrophy
{14485} myotonic dystrophy
{14488} myotonic dystrophy
{14491} myotonic dystrophy
On muscle biopsy, the pathologist sees:
* Another locus (CNBP / ZNF9, "proximal myotonic myopathy", "myotonic dystrophy type II, thankfully rare) results from tetranucleotide repeats at a different locus; genetically it is even more unstable than myotonic dystrophy type I. Since muscle involvement is rather mild, it is easy to overlook both clinically and on biopsy; pathologists see type II fiber atrophy and central nuclei (J. Neuropath. 67: 319, 2008). Heart disease (fibrosis, curious inclusions) and sudden death are prominent features.
FACIOSCAPULOHUMERAL DYSTROPHY
In this family of illnesses, the muscles of the face, shoulders, and upper arms are involved most severely.
The weird genetics was a major mystery for decades and was finally worked out for the common form ("FSHMD1A"). See Science 329: 1650, 2010. First, a region of repeats in the D4Z4 gene near the telomere becomes deleted. Second, the "dead / junk" gene DUX4 within the D4Z4 becomes reactivated.
As you'd expect from the genetics, the disease is of varying expressivity, and seldom lethal. Patients' shoulders and upper arms waste away, beginning in their teens or twenties.
Staining muscle with NADH reveals "moth-eaten" or "mottled" myofibers. Other changes are not usually striking.
{14515} facioscapulohumeral dystrophy, patient
![]() Facioscapulohumeral dystrophy
Facioscapulohumeral dystrophy
Wash U, St. Louis
LIMB-GIRDLE DYSTROPHIES
The hips and/or the shoulders are involved, and weakness leads to progressive disability sometime during adult life.
Muscle biopsy often shows central nuclei, but there are no specific findings.
* Most typically, the mutation is in calpain-3 ("LGMD 2A"; update Brain 128: 732, 2005), dysferlin ("LGMD 2B"; Neurology 56: 660 & 1472, 2001; Arch. Neuro. 64: 1176, 2007; Am. J. Path. 172: 774, 2008; Am. J. Path. 175: 1817, 2009; different allele produces a the distal "Miyoshi myopathy"), or one of the sarcoglycans (alpha-sarcoglycan = adhalin Nat. Genet. 11: 257 & 1266, 1995; 3 others known, update Neurology 67: 167, 2006). or POMT1 ("LGMD 2K"; wide range depending on allele: Neurology 66: 1564, 2006); a dystroglycan mutation NEJM 364: 939, 2011. ISPD (Brain 136: 369, 2013), In the less-common dominant forms, genes include myotilin, lamin A/C (update Neurology 78M: 1258, 2012), caveolin-3, and even collagen VI (several eponymous phenotypes depending on the mutation; as you'd expect, double-jointedness is common; Neurology 58: 593, 2002; Neurology 59: 920, 2002);
* Some caveolin-3 mutations produce the rare but picturesque "rippling muscle disease", with wiggly waves on percussion; Neurol. 57: 2273, 2001.
{14521} limb-girdle dystrophy, patient
{14385} limb-girdle dystrophy, histology
CONGENITAL MUSCULAR DYSTROPHY:
This is an enormous group of genetic diseases in which the child is weak from birth, may or may not have progression, and has muscles that show some of the histologic features familiar from the other muscular dystrophies. Several are well-characterized (update Arch. Neuro. 61: 189, 2004).
The deficiency is most often in merosin, a laminin-like protein; you can diagnose these on skin biopsy instead of going after muscle (Lancet 347: 582, 1996). Gene LAMA2 update Arch. Neuro. 62: 1582, 2005; Neurology 63: 1118, 2004.
* In "fiber type disproportion", type I fibers are much smaller than type 2 fibers. This is a feature of several known congenital myopathies, and others that are presently unclassified. In "uniform type I fiber disease", any of several known mutations cause all fibers to be type I (Neurology 70: 114, 2008 -- most often it's RYR1, as in "central core disease" where again type I fibers predominate -- Swedish series of the host of RYR1 mutations in Sweden Anesth. Analg. 111: 185, 2010). "Centronuclear myopathy", with just central nuclei and slow progression, can be caused by mutant dynamin II (DNM2; Brain 129: 1463, 2006).
* Mutations in collagen 6, which is in the endomysium anchoring it to muscle, give a mix of progressive congenital muscular dystrophy (myocytes undergo apoptosis for some reason) and hyperflexible joints (as in Ehlers-Danlos); they range from the severe Ullrich to the mild Bethlem myopathy (J. Med. Genet. 42: 108, 2005). Spot them by the baby being born with the feet flexed up against the shins -- why?
* Many other forms of congenital muscular dystrophy exist. Laminin deficiency: Neurology 55: 1120, 2000; a huge family of autosomal recessives called "dystroglycanopathies", with CNS and eye problems Neurology 69: 1254, 2007; Bethlem/Ullrich with mutated collagen VI (Neurology 69: 1035, 2007; Neurology 70: 1192, 2008); plectin (crosslinks intermediate filaments to their targets: Neurology 76: 327, 2011); MYL2 (Brain 136: 292, 2013), lots more. "The fukutinopathies" (two loci) often have associated distinctive brain malformations; they include a common Japanese childhood illness (Brain Dev. 31: 419, 2009).
OTHER HEREDITARY MUSCLE DISEASES ("the other congenital myopathies"; floppy babies or kids who do especially poorly in gym-class). This group does NOT show the histopathology suggesting muscular dystrophy.
You have already studied the glycogen storage diseases. For review:
POMPE'S DISEASE (glycogenosis II; acid maltase deficiency / glucosidase) produces floppy babies, big hearts, and often early death from cardiac failure; milder forms exist.
{15334} teen with mild acid maltase deficiency; looks okay but tires easily at sports
McARDLE'S DISEASE (glycogenosis V, myophosphorylase deficiency) is a mild disease. Glycogen bumps lie beneath the sarcolemma. The glycogen stores cannot be mobilized rapidly. Patients are poor athletes, and if they try or are forced, they get bad cramps and rhabdomyolysis. Genes: NEJM 329: 241, 1993.
* Tauri's glycogenosis VII / phosphofructokinase looks the same clinically.
* Glycogenin deficiency, a newly-discovered glycogen storage disease primarily affecting muscle and heart: NEJM 362: 1203, 2010.
![]() McArdle's Glycogenosis
McArdle's Glycogenosis
Brazil Pathology Cases
In Portuguese
* NEUTRAL LIPID STORAGE DISEASE is a rarity caused by inability to break down triglyceride droplets after they reach a certain size (Arch. Neuro. 69: 530, 2012).
MITOCHONDRIAL MYOPATHIES are inborn errors of metabolism that seem to primarily involve mitochondria. They feature defects in the pyruvate dehydrogenase complex, tRNA synthetases (probably most common, for example Neurology 44: 975, 1994), ATPase production, and the cytochromes (mitochondrial or autosomal inheritance, see Neurol. 44: 721, 1994). Some also involve the brain ("encephalomyopathies").
They include the mitochondrial-inherited Kearns-Sayre syndrome, with ophthalmoplegia, retinal pigmentation, cerebellar ataxia, and heart block. By now, dozens of distinct mitochondrially-inherited diseases affecting muscle are known, and drugs such as AZT and suramin produce acquired lesions that look similar.
The histologic hallmark of most of these illnesses is ragged red fibers. These are ragged because there are too many mitochondria, often abnormal ones, clustered around their edges under the sarcolemma. (* Future pathologists: See them best using Gomori trichrome stain.)
* The clever screening test is to have the patient pump the hand-gripper for three minutes; a very low pO2 in the venous blood from that arm suggests mitochondrial myopathy (Neurology 58: 1533, 2002).
On electron microscopy, the damaged mitochondria contain "parking-lot crystals" composed of abnormal creatine kinase (Proc. Nat. Acad. Sci. 91: 5089, 1994).
{14435} mitochondrial myopathy; mitochondrial clusters are dark purple
{14436} mitochondrial myopathy; mitochondrial clusters are
dark b;ie
* A mitochondrial myopathy that'll look normal on biopsy is mutated cytochrome C disease (NEJM 341: 1077, 1999). These patients have severe exercise intolerance and are likely to have lactic acidosis even at rest.
* Defects in carnitine metabolism include several obscure diseases (Pediatrics 84: 312, 1989; Am. J. Ob. Gyn. 170: 1390, 1994). Depending on the problem, muscle cells may be fat-laden or appear normal. There are no "ragged red fibers".
* Hereditary coenzyme Q deficiency features ragged red fibers, and responds dramatically to generous doses of supplemental coenzyme Q: Neurology 57: 515, 2001.
* A congenital mitochondrial myopathy caused by cytochrome C oxidase-deficiency sometimes self-cures during the first months of life depending on the mutation (Brain 132: 3165, 2009).
ROD MYOPATHY ("rod body myopathy", "nemaline myopathy"; "nema"- means "thread") is a family of autosomal-dominant (usually), non-progressive (usually) disorders with widely variable penetrance. The "nemaline rods" are masses of Z-band material (* notably actin).
* The best known locus is tropomyosin 3, another is actin (Nat. Genet. 23: 208, 1999); troponin tropomyosin 1 is another, and still another is tropomyosin 2 (Arch. Neuro. 64: 1334, 2007; Brain 136: 494, 2013).
{14376} rod body ("nemaline") myopathy
{14378} rod body ("nemaline") myopathy
{14379} rod body ("nemaline")
myopathy, Gomori trichrome stain
![]() Nemaline myopathy
Nemaline myopathy
Wash U, St. Louis
THE OTHER HEREDITARY ONES
* "Lipid myopathy" features fatty change as the major finding. Most of these people have a deficiency in carnitine palmitoyltransferase, and have weakness and rhabdomyolysis if they over-exercise (J. Neuro. Neurosurg. Psych. 62; 169, 1997.)
"Central core disease" is a group of variably-inherited, variably-severe, often non-progressive diseases featuring many muscle fibers with a full-length "central core" where there are no mitochondria and even the sarcomeres may be scrambled. There may or may not be a great preponderance of type I fibers. (Future pathologists: See it with the NADH tetrazolium reductase stain, or even PAS.) The most common gene is the ryanodine receptor, the intracellular calcium release channel (Neurology 59: 284, 2002; another allele and syndrome here Neurology 65: 1930, 2005).
* "Myotubular myopathies", variously inherited and variably severe, form another plethora of diseases. The deadly X-linked recessive form is caused by lack of good myotubularin, an ancient membrane protein (Nat. Genet. 18: 303, 1998, Nat. Genet. 13: 175, 1996.
* Desmin myopathy (desmin gene mutated): NEJM 342: 770, 2000.
* Spheroid body myopathy (mutated myotilin): Neurology 65: 1936, 2005.)
Myofibrillar myopathies are genetic diseases with dissolution of the sarcomeres beginning at the Z-disk. Masses of various muscle proteins may remain, but the structure is gone. Several are known (Neurology 62: 1363, 2004; Brain 127: 439, 2004; Brain 130: 3250, 2007; a myotilin allele and how it does its work Am. J. Path. 171: 1312, 2007; myotilin update Am. J. Path. 180: 1570, 2012). Filamin C (FLNC) myofibrillary myopathy: Brain 130: 3250, 2007; Neurology 75: 547, 2010; Brain 135: 2642, 2012.
* Myopathy with tubular aggregates are also genetic; the diagnosis is made on biopsy, and the aggregates are probably sites where muscle proteins exit the rough endoplasmic reticulum (J. Path. 207: 313, 2005).
{27319} central core disease; patient (no really diagnostic features visible)
{27331} central core disease; patient (no really
diagnostic features visible)
{27352} central
core disease; patient (no really diagnostic features visible)
{27325} central core disease, patient
INCLUSION BODY MYOSITIS ("distal myopathy with rimmed vaculoes"; Am. J. Path. 156: 1835, 2000; Am. J. Path. 164: 1, 2004):
A common hereditary (sometimes syndromic: Neurology 67: 644, 2006) or sporadic inflammatory-necrotizing myopathy. The sporadic form is usually seen in older adults; it involves especially the grip muscles ("The only problem is that I can't twist the caps off bottles").
The histopathology is distinctive. There are vacuoles containing (surprise!) phosphorylated tau twisted as paired helical filaments, just like the tangles in Alzheimer's, along with some other proteins from the neuropathology unit including prion precursor protein, parkin and apoprotein E. It stains as amyloid.
In fact, the biochemistry seems similar in many ways to the changes in Alzheimer's (Neurology 66(2 S 1): S-39, 2006), and it is being called a "myodegenerative disease".
The vacuoles look autophagocytic, and when these cells are grown in culture, they auto-phagocytize (Am. J. Path. 177: 1377, 2010).
* It is basically not treatable, and is notoriously unresponsive to anti-inflammatory medicines. See Neurology 45: 1302, 1995. The first report of an response was to alemtuzumab (anti-mature B and mature-T cells; Brain 132: 1536, 2009).
* The hereditary form results from lack of one of the carbohydrate-processing enzymes (Neurology 59: 451, 2002; update on alleles and diagnosis Neurology 75: 265, 2010).
RHABDOMYOLYSIS
Sometimes myoglobin leaks out of skeletal muscle. This may be acute or chronic.
Some normal people get rhabdomyolysis after exercise. If you're out of shape and overdo it, you'll probably experience mild rhabdomyolysis (ouch!) If severe, you might have glycogen storage disease (V or VII), or some other unusual problem. We might hypothesize pH-related cell injury, but details are obscure.
STATIN MYOPATHY is rare but very important: JAMA 289: 1681, 2003. People on the familiar cholesterol-lowering medications develop rhabdomyolysis. A fatal case after many years on statins Am. J. Card. 99: 1171, 2007. Please don't miss this -- statins are very widely used, rhabdomyolysis is rare, and your patient may simply "feel sore", which is of course also very common. We still don't know how it happens -- watch for a susceptibility gene or two soon, a finding that will most certainly impact daily practice.
Other causes of rhabdomyolysis include crush injury, electrical injury, heat stroke, motor seizures, cocaine abuse, methamphetamine abuse, malignant hyperthermia (see below), neuroleptic malignant syndrome (from the strong dopamine D2-blocking anti-psychotic drugs), long-term glue sniffing (J. Tox. 38: 679, 2000), certain snake venoms (Brain 133: 3181, 2010), or acute systemic viral illness (H1N1 JAMA 302: 1863, 2009.
ALCOHOLIC RHABDOMYOLYSIS / MYOPATHY is a minor mystery of medicine when it occurs apart from obvious trauma (Minn. Med. 71: 769, 1988). Some (but probably not all) of the explanation is that alcoholics (and dopesters) get ischemia of skeletal muscle by not shifting their weight (i.e., people who are passed out don't fidget, toss, and turn like we do.)
Markers for rhabdomyolysis are the same as for any other disease that releases the contents of myofibers. Myoglobin appears in the urine, and the "muscle enzymes" (creatine kinase, aldolase, SGOT, others) rise in the serum.
Large amounts of myoglobin in the glomerular filtrate tend to precipitate in the kidney tubules. This pigment nephropathy is troublesome but seldom lethal.
Regardless of cause, muscle biopsy in "rhabdomyolysis" shows degenerating and regenerating fibers, with macrophages around them, but no lymphocytes or other inflammatory cells.
![]() Lovastatin / niacin rhabdomyolysis
Lovastatin / niacin rhabdomyolysis
Pittsburgh Pathology Cases
This might be a good place to mention MYOSITIS OSSIFICANS, in which endochondral bone formation occurs within the muscular connective tissue.
Localized myositis ossificans follows trauma and probably represents bony metaplasia of scar ("myositis ossificans traumatica"). Pathology of the developing lesions: Clin. Ortho. Rel. Res. 403-S: S-110, 2002.
PROGRESSIVE FIBRODYSPLASIA OSSIFICANS (formerly "generalized myositis ossificans") is a dreadful disease in which new cross-links form across the joints, rendering them immobile. These patients' skeletons end up in pathology museums.
{27349} myositis ossificans; bumps are bone
![]() Myositis ossificans
Myositis ossificans
Pittsburgh Pathology Cases
On your surgical rotations, you'll learn about the various COMPARTMENT SYNDROMES, in which swelling (especially from reperfusion of muscle ischemic for some other reason) within one of the deep compartments of an extremity interferes with venous drainage and causes infarction.
INVOLVEMENT OF MUSCLE IN SYSTEMIC DISEASE
![]() Ipecac myopathy
Ipecac myopathy
Pittsburgh Pathology Cases
Probably the most common myopathy you will see (and probably ignore) is alcoholic myopathy. Biopsy that scrawny drunkard's muscle, and you'll find fibrosis between the fibers, and hypertrophy of the remaining fibers (i.e., many fibers are long-gone). They are mostly the ones that also have the alcoholic cardiomyopathy (Ann. Int. Med. 120: 529, 1994).
You are already familiar with the catastrophic clostridial infection GAS GANGRENE, in which muscle is prominently involved.
* PYOMYOSITIS, bacterial infection of muscle, usually follows a break in the skin, usually in a younger person who has some immune compromise. The diagnosis is made on imaging; in the USA, resistant staph are dangerous, and abscesses may form. You are also familiar with TRICHINOSIS (trichinellosis), in which worms encyst and die in the muscles (they seek the busiest and best-perfused, i.e., the diaphragm and external eye muscles).
Lots of granulomas in the muscle probably indicates SARCOIDOSIS. Twice I've picked up POLYARTERITIS NODOSA (surprise!) on muscle biopsy.
The virus that attacks muscle most aggressively is probably COXSACKIE B virus![]() ;
also remember DENGUE. Myositis contributes to the agony of
TYPHUS
;
also remember DENGUE. Myositis contributes to the agony of
TYPHUS![]() .
.
* "White muscle disease", from selenium deficiency, is mostly a veterinary problem, but is seen occasionally in malnourished people (Neuro. Neurosurg. Psych. 67: 829, 1999).
* You'll need to decide for yourself about "macrophagic myofasciitis", sheets of macrophages within skeletal muscle but without muscle damage; clearly a persistent local reaction to aluminum adjuvants in vaccines (Med. J. Aust. 183: 145, 2005; J. Child Neuro. 23: 614, 2008; Neuromusc. Dis. 16: 347, 2006); the local macrophages contain aluminum hydroxide. Patients with "biopsy-proven macrophagic myofasciitis" can have pretty much any generalized illness. Common sense would suggest that we just happened to biopsy an old injection site, and the patient has something else, too (Ultrast. Path. 31: 45, 2007). Of course, the anti-immunization community considers it to be the cause of chronic fatigue syndrome and multiple sclerosis (Brain 124: 974, 2001) and probably everything else.
{46215} pus in necrotic muscle infected with bacteria; this is unusual
{08215} trichinosis
{08288} trichinosis
{15750} trichinosis
{24498} trichinosis
|
|
During "immunopathology", you'll study the miserable POLYMYOSITIS-DERMATOMYOSITIS ("idiopathic inflammatory myositis", review Lancet 335 53, 2000). Worth reiterating:
In polymyositis, the immune attack is on the myofibers themselves. The myofibers express HMD1 antigens on the sarcolemma, which is abnormal.
In dermatomyositis, the immune attack is on the muscle microvasculature.
Selective atrophy of the muscle fibers at the edges of the fascicles is very characteristic of dermatomyositis, even if there is no inflammation or necrosis.
In either disease, patches of chronic inflammation are typical, and you may see injured or dying fibers.
HIV infection at any stage can simulate polymyositis (Arth. Rheum. 49: 172, 2003).
{29501} polymyositis, histology
{05780} polymyositis, histology
{09039} polymyositis, histology
{14352} polymyositis, histology
{14356} polymyositis, histology; obvious perifascicular atrophy
{14358} polymyositis, histology; obvious perifascicular atrophy
{14433} polymyositis, really bad
inflammation
{29504} polymyositis, histology, showing regeneration
![]() Dermatomyositis
Dermatomyositis
Nice muscle biopsy photos
Oklahoma
![]() Childhood dermatomyositis
Childhood dermatomyositis
Wash U, St. Louis
![]() Adult dermatomyositis
Adult dermatomyositis
Wash. U., St. Louis
Illustrated notes
The most characteristic autoantibodies are directed against several of t-RNA synthetases (J. Immunol. 144: 1737, 1990). Anti-Jo-1 (anti-histidyl-tRNA synthetase) was the first of these antibodies, which are considered markers for polymyositis & perhaps pulmonary fibrosis. However, these occur only in a minority of cases.
In a large minority of cases, the disease is the first sign of an internal malignancy, especially ovarian cancer.
POLYMYALGIA RHEUMATICA (Lancet 381: 28, 2013; BMJ 336: 765, 2008)
A poorly understood but important disease, affecting perhaps 1 out of 1000 folks over age 50. Almost all patients are older adults, and a majority are women. Around 30% also have temporal arteritis (if you ask and/or palpate). There is pain and morning-stiffness in the neck, shoulders, and hips. Physical exam and routine labs are otherwise singularly un-diagnostic. The pathology is really more in the synovium and bursa than in the muscles (Arth. Rheum. 44: 115, 2001). Erythrocyte sedimentation rate is often, but not always, high; the same is true of C-reactive protein. The treatment is low doses of systemic glucocorticoids, which works in a few days, and patients are grateful.
It's worth mentioning once again that temporal arteritis is "the prime medical emergency in ophthalmology" (Med. Clin. N.A. 97: 329, 2013).
* The link to the very common HLA-DR4 is established; the relationship to a previous viral or chlamydial infection less so.
CRITICAL ILLNESS MYOPATHY ("acute quadriplegic myopathy" was the original name for the group of illnesses; there are now many other names, first major review; Crit. Care Med. 27: 2544, 1999; updates Muscle and Nerve 23: 1785, 2000; Muscle Nerve 32: 140, 2005); Chest 131: 1541, 2007
Recently recognized as more-than-just-atrophy. It first came to be recognized when patients on systemic glucocorticoids for emphysema (yeah) or severe asthma or other illnesses would develop profound weakness and pain, of relatively abrupt onset (Am. J. Resp. Crit. Care Med. 153: 1958, 1996). Soon it was noted that administration of paralyzing agents to steroid-treated people already on the respirator seems to precipitate the disease (Am. J. Resp. Crit. Care Med. 153: 1686, 1996; Neurology 46: 600, 1996). It was noted that some these patients never got their strength back.
* Medical terminology buffs: "critical illness" seems to be variably defined, but with some failure of multiple organs already evident and "systemic inflammatory response syndrome" presumably present (Muscle Nerve 2005 op cit blames the multiple lines and intubation in patients in the ICU for over a week).
In the original biopsy studies of the entity that we came to call "acute necrotizing myopathy of intensive care" (i.e., the one that doesn't get better), pathologists observed:
After much study, today's pathologists divide "myopathy of critical illness" into several subtypes, which may occur together.
Probably these illnesses have always been with us, but we are only noticing them because of better survivals by victims of catastrophic illness. In fact, a large majority of patients in the ICU have some degree of myopathy if you do direct muscle stimulation (JNNP 77: 500, 2006); about half will also show the neuropathy.
THICK FILAMENT MYOPATHY is striking, both on H&E and on electron microscopy. Myosin, but not actin, disappears (Neurology 55: 854, 2000). The typical patient is an asthmatic who suddenly got much worse and had to be put in a ventilator. Patients usually got glucocorticoids and/or NJM blockers. Occasionally it follows sepsis. Most patients recover if the underlying illness is treated successfully.
As you'd expect, ACUTE NECROTIZING MYOPATHY OF INTENSIVE CARE features vacuolization, necrosis, and phagocytosis of muscle fibers. Expect weakness, very abnormal electromyography, a greatly elevated creatine kinase, and a poor outcome. Thankfully, it's rare.
In ACUTE RHABDOMYOLYSIS, the clinical picture will be similar to the acute necrotizing illness, but electromyography will be near-normal. Also uncommon, no one understands why it occurs in ICU patients at all; again, NMJ blockers and glucocorticoids seem to precipitate it.
DISUSE MYOPATHY (a term that's passing out of use) is simply the weakness that develops in unused muscles over time. Remember that type II fibers atrophy more than type I's.
We will cover the better-understood CRITICAL ILLNESS POLYNEUROPATHY, another weakness syndrome that may well be present in these patients as well, when we talk about peripheral nerve disease. It evidently results from the systemic inflammatory response syndrome, familiar from general pathology.
In the meantime, loss of movement in a comatose ICU patient may not mean deterioration in brain function (Lancet 347: 1579, 1996 pointed out the obvious). The question of whether muscle biopsy is indicated depends on the big picture.
* Possible molecular mechanisms and prevention with evoked muscle contraction: Am. J. Resp. Crit. Care Med. 187: 387, 2013.
Confusing: "Steroids" in the muscle literature as elsewhere means either glucocorticoids or androgens (see below).
Chloroquine is notorious for producing a myopathy with vacuoles in muscle cells (no marvel; chloroquine exerts its major effects on lysosomes). For the biochemistry, see J. Biochem 131: 647, 2002.
* "Reducing body myopathy", a progressive disease with granules that reduce nitroblue tetrazolium in the muscle fibers has been linked to FHL1, on the X-chromosome (Brain 132: 452, 2009).
THE MUSCLE MEMBRANE DISEASES: Electrical troubles! Old review: NEJM 328: 482, 1993. The chloride channel itself: Neurology 54: 937, 2000. Reliable stain Neurology 79: 2194, 2012.
Chloride channel disease -- MYOTONIA CONGENITA: several inherited diseases with excessive muscle tone (i.e., impaired ability to relax after forceful contraction).
Patients often have considerable muscle hypertrophy and strength, excelling at sports where strength is more important than speed; some (not all) forms eventually cause atrophy. The histology is usually normal or nearly so.
* Goats with myotonia congenita are bred for their superior meat; they are also the animal model (Neuromusc. Disorders 10: 160, 2000).
|
{14500} myotonia congenita with hypertrophy
{14503} myotonia congenita, older patient with atrophy {14506} myotonia congenita, older patient with atrophy |
|
The usual gene for both the common dominant (Thomsen's mild disease * Thomsen had it) and recessive (Becker's more serious disease, not to be confused with Becker's dystrophy) have been found at the CLC-1 ("chloride channel 1") locus (Science 257: 797, 1992; update on this very complicated gene with 23 exons Brain 125: 2392, 2002).
Stay tuned for the discovery of several more alleles here that determine why some guys "naturally" have much bigger muscles than other guys (i.e., it's not just your testosterone or your "bone structure", dudes).
Myotonic dystrophy, of course, also features an electrical disturbance; the gene involves a membrane component.
PERIODIC PARALYSIS (Brain 129: 8, 2006):
Several hereditary (usually autosomal dominant) channelopathy diseases, which feature striking episodes of paralysis without clouding of consciousness.
Precipitated respectively with low, normal, and high serum potassium. Most seem to respond to carbonic anhydrase inhibitors, and pathologists seldom see them. Probably some of them go into the SIDS "we don't know exactly why" category.
Hypokalemic periodic paralysis type I is a dominant calcium channel mutation (Am. J. Hum. Genet. 56: 374, 1995). Type II is a dominant sodium channel (CACNA1S: Brain 125: 835, 2002; Neurology 53: 1932, 1999; Neurology 57: 1323, 2001). Alleles at SCN4A (a sodium channel originally discovered as a cold-sensitive paramyotonia congenita locus) can produce it.
Anderson's (periodic paralysis, sudden death) is a potassium channel (KCNJ2) mutation: Circulation 105: 2592, 2002.
Hyperkalemic periodic paralysis (much less common than the hypokalemic variant) and potassium-aggravated myotonia are usualy caused by a differently-mutated SCN4A (J. Neurosci. 19: 4762, 1999). More mutations Neurology 44: 1500, 1994. Yet another allele: Arch. Neur. 51: 1095, 1994).
* There is also a dominant potassium channel (KCNE3) disease that expresses itself best in the presence of hyperthyrodism; don't know why (J. Clin. Endo. Metab. 87: 4881, 2002).
* Survey of England's channelopathy patients (periodic paralysis and nondystrophic myotonia): Neurology 80: 1472, 2013.
MALIGNANT HYPERTHERMIA SUSCEPTIBILITY
Some people (around 1 in 5000), when they go under a general anesthetic, develop rhabdomyolysis, acidosis, elevated core temperature, and/or serious heart rhythm problems.
The ability to get this is hereditary, usually autosomal dominant. The mutations are in the voltage-gated calcium channels in skeletal muscle; * the most common locus is RYR1, ryanodine receptor; Lancet 352: 1131, 1998; recessive Neurology 59: 284, 2002; molecular mechanisms Brain 130: 2024, 2007.
* Update on how to screen: JAMA 293: 2918, 2005 (concludes that you really can't).
* There are a host of other channelopathies, notably those that cause sudden cardiac death or epilepsy. Pathologists hate them as they have no gross or microscopic lesions. More soon.
OTHER MUSCLE PROBLEMS
MYOFASCIAL PAIN SYNDROMES (Arch. Phys. Med. Rehab. 83 (3S1): S40, 2002; Am. Fam. Phys. 65: 653, 2002) are presently a major mystery of medicine.
The problem is electrophysiological (Am. J. Phys. Med. 81: 212, 2002). The connection between these nodules, TMJ syndrome, fibromyalgia, interstitial cystitis, and so forth will be clarified someday. No one knows the anatomic pathology.
Acupuncture fails totally: Arch. Phys. Med. Rehab. 82: 986, 2001; botox offers some hope (Arch. Phys. Med. Rehab. 84 3S1: S69, 2003); electronic muscle stimulation helps (Am. J. Phys. Med. Rehab. 76: 471, 1997) and is now standard (Med. Clin. N.A. 91: 229, 2007).
EOSINOPHILIA-MYALGIA SYNDROME
This was a myositis (etc., primarily a vasculitis, and with scleroderma-like skin changes), with severe pain and weakness, seen in people who took a certain brand of L-tryptophan tablets from the "health-food" industry in 1989. Circulating levels of eosinophils were very high, and eosinophils and their debris were abundant in the damaged tissues.
The cause was the impurity 1,1'-ethylidenebis[tryptophan]. Review: Mayo Clin. Proc. 66: 535, 1991). See also South. Med. J. 83: 675, 1990; Chest 97: 1032, 1990; NEJM 322: 869, 1990; Hosp. Pract. 27(4A): 65, April 30, 1992.
* Don't worry about similar, rare diseases (eosinophilic fasciitis, the does-it-exist-or-not "human adjuvant disease" following breast implants, etc.)
![]() Rhabdomyoma
Rhabdomyoma
Pittsburgh Illustrated Case
* RHABDOMYOSARCOMA gets covered under bone tumors and sarcomas.
{24748} rhabdomyosarcoma (striations)
{09006} alveolar rhabdomyosarcoma; very undifferentiated tumor
{25305}
sarcoma botryoides with cambium layer
![]() Rhabdomyosarcoma
Rhabdomyosarcoma
WebPath Photo
 Action hero -- 1950's Kirk Douglas as "Spartacus" |
 Action hero -- 1980's |
ATHLETICS
Sports do not build character. They reveal it.
-- Heywood Hale Broun, TV commentator
Muscles are fun. Athletes push their bodies to extremes seldom seen even in disease.
* At Northwestern, we had a histotechnologist who ran 16 miles to and from work daily. It was fun introducing him to clinicians and having them "check out his heart".
* In ancient Greece, divided by geography into small regions ("city-states" -- each looking out for themselves), every man of fighting age had a duty to himself and his community to be physically fit for military service and hand-to-hand combat, as your city's neighbor could attack at any time. Hence the "gymnasium", where guys would work out. "Gymnos" means "naked"; the Greeks didn't have workout apparel and didn't want to stink up their street clothes. The men also did not have automobiles or power tools to talk about, so conversation "between sets" turned to ideas and the birth of much of what's still best about our world.
| Aerobic
training ("getting in shape") involves repetitively forcing the muscle to maximum metabolic demands. Aerobic exercise: Science 276: 1325, 1997. You measure aerobic fitness by how much oxygen you can use, for your size, in a minute. Aerobic training changes a number of parameters. Perhaps the most important is an increased mitochondrial activity in both type I and type II fibers (Am J. Physio. 278:E-153, 2000). Glycolytic enzymes are increased, and there is also talk of increased numbers of capillaries. Different isoforms of the myosin heavy chain seem to reappear that are more efficient than those in senentary adults.
The best-established finding in aerobically-trained muscle is the increase in lactate transporter on both mitochondria and sarcolemma; I hope this is not a surprise (Am. J. Phys. 278: E571, 2000; Eur. J. Appl. Phys. 96: 636, 2006). It's now clear that how much you can improve this by exercising is genetically determined (J. Clin. Endo. Metab. 92: 1927, 2007). A variety of other ways in which glycolysis, fat-burning, and oxidative phosphorylation are increased in trained muscle are known; they must have something to do with why insulin sensitivity increases (J. Appl. Phys. 111: 427 & 1554, 2011; lots more recently). |  |
Unless the muscle is working against resistance, don't expect to see a significant gain in muscle mass or strength. Muscle responds to resistance training by adding new fibers to the individual sarcomere units. "Aerobically conditioned muscle" has altered mitochondria that are much more effective, but does not undergo hypertrophy.
Of course, the changes of the aerobically-trained person are not confined to voluntary muscles. The muscle that is most affected by aerobic training is the heart. It undergoes hypertrophy (which is good in this instance; it can also beat slower). Claims of "improved lung function" are hard to demonstrate, but the shapes of marathon runners' chests do change to improve air supply. Ask a trainer about carbohydrate-loading to increase muscle glycogen stores (and thereby endurance) before the big race.
Being aerobically fit clearly is a powerful way of forestalling the onset of type II diabetes (Ann. Int. Med. 143: 251 & 323, 2005); the studies are getting more and more impressive.
* How does exercise help your lipoproteins? This year, the explanation goes like so: (1) exercising muscle's lipoprotein lipase selectively removes triglyceride from VLDL's; (2) this shrinks them and cholesterol molecules fall off the surfaces; (3) and the cholesterol ends up on HDL.
* Being fit helps older folks sleep better, etc., etc., etc., JAMA 277: 32, 1997. Overweight older folks benefit from a combination of diet and exerise; doing both is better than either alone (well, go figure, but the study shows you can get them to comply): NEJM 364: 1218, 2011. Benefits of fitness training for those with congestive heart failure: J. Am. Coll. Card. 58: 561, 2011; Lancet 380: 294, 2012 (helps measurably against depression in this depression illness).
We're still reading studies that "show" the benefits of exercise to be tremendous (for example, JAMA 273: 1093, 1995 measured aerobic fitness and found an 8x reduction in coronary mortality, and an overall mortality reduction of 44%; similar Lancet 352: 759, 1998). Before you embark on your own aerobic fitness program, reflect that (1) being sick lowers your aerobic fitness, and (2) being sick in the first place makes it less likely that you will exercise, and (3) people who exercise have other healthier habits. Of course you cannot control for these in a prospective study.... The retrospective review in JAMA 276: 205, 1996 struck me as more credible, and the benefits are almost certainly real.
NIH consensus statement about physical-fitness and cardiovascular health: Am. Fam. Phys. 54: 763, 1996, JAMA 276: 241, 1996. The Surgeon General: JAMA 276: 522, 1996.
* Uncle Sam spends megabucks on "the primary prevention of heart disease" at the grammar school level, including extensive indoctrination of the kids, and ends up proclaiming triumphantly that kids in the study group (i.e., who'd been told at length what Uncle Sam wanted them to say) reported reducing their percentage of fat calories by a whopping 2%, and self-reported exercising 12 more minutes a day than controls. Uncle Sam also compared body size and cholesterol levels (no difference) but Uncle Sam did not bother actually measuring adiposity, muscularity, or physical fitness. Somehow this was actually published: JAMA 275: 768, 1996. More from Uncle Sam: He spent more money in 1996 and discovered that most fat people do not exercise much during their leisure time (JAMA 275: 905, 1996), wow. In 1998, still more of your tax money went to show that kids who watch more TV exercise less and are fatter! The authors wanted more money so they could spend it on health promotion (JAMA 279: 938, 1998), uh huh. Update: Yes indeed, fat kids exercise less (JAMA 307: 704, 2012).
Muscle strength training ("getting bulked up") involves overcoming resistance, typically "pumping iron".
Muscle strength is proportionate to muscle mass. A large limb muscle can lift about 3 kg/cm2 of its maximum cross-sectional area. The amount of load that a muscle can hold steady is around 40% greater than the amount it can lift. A very strong man can exceed the force holding the tendons to the bone. Ruptures of the biceps and other tendons are not uncommon.
A person's muscle mass ("muscle bulk") is determined by a combination of heredity (* probably including differences in base muscle tone and the genetic markers listed below), personal average androgen levels (widely variable even among people of the same age and gender), and the strength demands placed on the muscle.
* You may learn in Physiology how trained skeletal muscle (resistance, endurance) changes its myosin heavy chain isoforms. That the Akt/mTOR pathway is key to adding protein fibers to sarcomeres in response to mechanical loading has been known for some time (Nat. Cell Bio. 3: 1014, 2001.)
It is now well-established that resistance training causes satellite cells to differentiate as myocytes and become incorporated into myocytes; the idea that it is "only hypertrophy" is simply wrong (Brain 131: 2832, 2008). They contribute nuclei to the growing myocytes (Cell Metab. 15: 25, 2012.)
By contrast, "muscle definition" ("getting trimmed / ripped / cut") results from both muscle bulk and (more important) lack of subcutaneous fat. Much sought-after, bodybuilders diet and do even aerobic exercise before shows or photos. It is probably not possible to "spot-reduce" fat from one portion of your body, and be skeptical when someone tells you a particular exercise is "particularly good for definition".
As noted above, an aerobically-trained adult also has about one liter more blood, which helps an "athletic-cut" person look "vascular" too. Again, much sought-after (contrast anorectics and zero-bodyfat "heroin chic" addicts).
 Age 34 |
I look like a rock quarry that someone has dynamited.
|
 Age 50 |
| As I predicted in 2001, the study of the serum autocrine factor "myostatin" has become
central to the field of muscle physiology (Science 296:1486, 2004).
The hormone enables fat production and muscle atrophy.
Belgian Blue cattle, which are lean and grotesquely muscled,
lack myostatin (Nat. Genet. 17: 71, 1997).
So are knockout mice lacking this protein (Proc. Nat. Acad. Sci. 98: 9306, 2001),
and there's now a homozygous child lacking the myostatin receptor
(Liam Hoekstra; NEJM 350: 2682, 2004 -- Mom
and her family are strength athletes, surely heterozygotes; originally Mom would not
say who Dad was, and the "pop" sources are still quiet). |
|
It is also possible to blockade myostatin in a mouse model, either genetically or with a monoclonal antibody (Am. J. Path. 168: 1975, 2006). The latter is just coming into use in the sports-doping community -- definitely stay tuned.
"Supraphysiological doses of testosterone" (NEJM 335: 1, 1996) and resistance training both (and especially together) cause hypertrophy of the fibers (type II fibers in every sport, type I's when endurance is a factor), with increases in the numbers of myofilaments and even sarcomeres.
We now know that, despite traditional teaching, a weight-lifter's muscle fibers may divide, or (more important) new fibers form from satellite cells. ("Muscles have a memory" after all. See Anat. Rec. 233: 178, 1992; Med. Sci. Sport 31: 1528, 1999.)
The key to building bulk is (1) lifting heavy weights (today's trainers recommend 3 sets of 6-10 repetitions of your maximum weight, three times a week), and (2) anabolic steroids (your own male hormones, or see below.) A man who lifts weights several times a week is likely to increase his muscle mass by around 30% after eight weeks. This will impress his male buddies and perhaps even a few women.
Some men bulk up much more easily than others do. Gym types talk about "easy gainers" and "hard gainers". The genetics of this is just coming clear. One locus is the angiotensin-converting-enzyme gene (where the allele seems to determine how much muscle you build in response to strength training): Lancet 353: 541, 1999; J. Clin. Endo. Metab. 86: 2200, 2001). Another is IGF-1 (J. Applied Physio. 98: 2147, 2005) Watch for variations in the myogenic proteins (such as "herculin"/Myf6/MRF4) to explain differences from person to person. You can read on your own about changes in myosin heavy chain subtypes in resistance-trained muscle, and so forth.
Far more men work out with weights today than in past decades. This is probably healthy, and it has also changed the image of what a fit man is expected to look like (Am. J. Psych. 162: 263, 2005). Compare yesterday's action-hero macho-man actors with today's gentle-ordinary-guy actors; the old pictures of Superman with the new ones; and even GI Joe's from the 1960's with today's models.
{18664} "pumped"
The traditional wisdom in "exercise and the heart" was to emphasize the health-benefits of aerobic training, and to dismiss the idea that strength training has benefits beyond sports. This all changed in the 1990's. Strength training helps old folks walk farther (Ann. Int. Med. 124: 568, 1996), re-muscles the elderly so they can do more ("reversing sarcopenia", Geriatrics 51: 46, 1996), strengthens rheumatoid arthritis patients and causes them to report less pain and less fatigue (Arth. Rheum. 39: 415, 1996), reduces (!) osteoarthritis activity in the knee (Nsg. Res. 45: 68, 1996), lowers diastolic blood pressure in older folks (Arch. Int. Med. 165: 756, 2005), "tells a counterstory of aging that resists the narrative of decline" (i.e., lets the world know you're not going to just give up, get old and die; J. Geront. 66: 628, 2011), etc., etc. Even the fibromyalgia patients benefit significantly (Arth. Rheum. 47: 22, 2002). Reports on strength training and lipids are mixed, but in 2007, the American Heart Association gave a reasoned, very extensive endorsement to resistance training for people both with and without heart diseases (Circulation 116: 572, 2007). Weightlifting builds and strengthens older folks (60+). J. Ger. Mar. 1995; Am. J. Phys. Med. Rehab. 81(S-11): S3, 2002). Older diabetics: J. Ger. 58: 740, 2003. Both resistance training and aerobic training reduce HgbA1c in diabetics (JAMA 305: 1790, 2011).
The academicians finally got around to seeing whether having
post-polio
* Weightlifting seems neither to help nor hurt myotonic dystrophy patients, while it apparently helps some neuropathy patients (Arch. Phys. Med. Rehab. 76: 612, 1995). Hopefully to no one's surprise, resistance strength training was very helpful for folks who have trouble walking because of peripheral vascular disease -- probably by improving the availability of the muscle. What's more, resistance training bulks the heart (Cardiology 90: 145, 1998) as aerobic exercise does. This was so politically incorrect that at first all the big-hearted bodybuilders in the study were wrongly accused just on this evidence of taking anabolic steroids. Science is now winning out over politics, at least here.
Lifting is safe, even for younger kids if you supervise them properly (Sports Med. 15: 389, 1993); I'd be concerned about using heavy weights that might cause premature closure of the epiphyses. It's safe for the emphysema folks (it makes them feel better! Thorax 47: 70, 1992), and the coronary-disease guys (Am. J. Card. 71: 287, 1993; Am. J. Card. 67: 939, 1991). The skeletal muscle mass of a distance runner is around 38% of body weight; for a bodybuilder, it's around 59% (J. Sports Sci. 11: 3, 1993). Bodybuilders will ask you for your opinions about various nutritional supplements to enhance their performance. Despite the advertisements, the ones that got tested during the 1990's were all total flops (animo acids: Int. J. Sport. Nutr. 3: 290, 298 & 306, 1993; boron: Int. J. Sport. Nutr. 3: 140, 1993; chromium picolinate Int. J. Sport. Nutr. 2: 343, 1992; growth hormone J. Appl. Phys. 74: 3073, 1993; I could only get these as abstracts). So what works? The value of both creatine (J. Fam. Pract. 51: 945, 2002; Am. J. Clin. Nutr. 72(S2): 607-S, 2000) and post-exercise intake of protein or carbohydrate are now established (Can. J. Appl. Phys. 25: 254, 2000.) More than 20&ngsp;grams of protein after working out is a waste (Am. J. Clin. Nutr. 89: 161, 2009). Creatine evidently makes the satellite cells divide (Int. J. Sports Med. 21: 13, 2000). Early concerns about creatine producing rhabdomyolysis seem to have come to nothing. Creatine is now being used to prevent muscle wasting during, and restore muscle mass after, immobilization (Diabetes 50: 18, 2001). No offense to anybody, but eating meat (rather than just other animal or vegetable proteins) helps too (Am. J. Clin. Nutr. 70: 1032, 1999). While lifting weights, it's best to keep your glottis open, and not Valsalva. The more elaborate instructions about "when to breathe in, when to breathe out" are of course designed to make lifters keep their glottis open.
* The unfortunate man who didn't know what was really in his "protein health drink" prepared specially at the gym: Br. Med. J. 313: 100, 1996. * Today, senior bodybuilders are much sought-after as supposedly possessing arcane knowledge about anabolic steroids, and there is a huge underground literature, much of which strikes me as dubious. Review (finally) in Sports Med. 32: 285, 2002, by the psychiatrists at Western Missouri. Weightlifting and 'roids for the men with AIDS wasting (wasting can proceed even if you are on HAART): JAMA 281: 1282, 1999. 'Roids help the man on dialysis stay well-muscled and well-functioning: JAMA 281: 1275, 1999. For the women: Arch. Int. Med. 165: 578, 2005 (seems safe and effective). They work. Men (South. Med. J. 84: 552, 1991, and also women; see Am. J. Ob. Gyn. 165: 1385, 1991) can and do develop spectacular muscles using steroids, and the drugs also improve mood and increase aggressiveness (JAMA 269: 2760, 1993 for the first placebo-controlled study; one guy in the subject group went crazy).
Users are willing to take the risks, which include:
The first six are common. In addition, women are likely to grow thick hair on their faces and other un-feminine places, and smell as bad as we men do because of the hypertrophy-hyperplasia of the apocrine glands. Pee-yoo! You have been warned.
Between 5% (Am. J. Dis. Child. 144: 99, 1990) and 11% (Pediatrics 83: 921, 1989) of high school athletes have used anabolic steroids. One older study cites 7.6% of high-school males and 1.5% of high-school females (!; Am. J. Dis. Child. 14: 823, 1992). Parents request them for their skinny, non-athletic sons (Pediatrics 84: 940, 1989). More recent self-reports (now that there's more of a stigma), it's only 1.5% of all teens but with no change between 1999 and 2004 (Pediatrics 119: 476, 2007); or 2.7% of twelfth-graders (Am. J. Phys. Med. Rehab. 88: 192, 2009 -- the retrospective study retired football players -- there are obviously lots of confounding variables; the 'roid users had more ligament injuries but not tendon injuries -- any ideas why?). We won't talk about college, Olympic, or professional athletes. In amateur boxing, which is primarily about speed and smarts rather than strength, and where keeping one's weight down is critical, there is probably little anabolic steroid use. In a switch from complete condemnation, the pediatricians (Pediatrics 99: 904, 1997) now talk about moderate steroid use as a personal choice for the young athlete (though of course it's probably illegal and immoral). Today's common-sensical doctor is invited to review the risks and remind Junior that the social benefits of jocking it up (i.e., excelling on team sports and looking a lot better than most other boys nowadays) can be obtained about as easily without using steroids. Common sense triumphant. More common-sensical advice for realist-physicians: Ped. Clin. N.A. 54: 771, 2007. The "official" statement from the American Academy of Pediatrics of course still condemns the use of all performance-enhancing substances (Pediatrics 115: 1103, 2005), and I think this is the moral thing to do. However, I'd much rather have my own son express an interest in trying steroids under supervision than telling me he has a favorite brand of beer, smoking tobacco, or getting a motorcycle. The politics of anabolic steroid use, and attempts at control: NEJM 321: 1042, 1989; the latter have historically been a joke (older review NEJM 322: 775, 1990; Olympics Nature 407: 124, 2000). Only six athletes were disqualified on screening for the 2008 Beijing olympics because of banned substances; six athletes were caught during the games. The Olympics folks now freeze blood samples for eight years, in the hopes that future technology will detect what we can't today. Truth be told, I have known a few gym guys who have tried anabolic steroids, and all regretted it in the long run. And in my unscientific series, most women prefer a naturally-muscled man.
{14612} skeletal muscle, normal
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about the pathology of skeletal muscle to consult these standard textbooks.
Dubowitz's Muscle Biopsy: A Practical Approach Robbins and Cotran Pathologic Basis of Disease Rosai and Ackerman's Surgical Pathology Rubin's Pathology: Clinicopathologic Foundations of Medicine Demay's Cytopathology In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request
Teaching Pathology
Ed's Autopsy Page Notes for Good Lecturers Small Group Teaching Socratic Teaching Preventing "F"'s Classroom Control "I Hate Histology!" Ed's Physiology Challenge Pathology Identification Keys ("Kansas City Field Guide to Pathology") Ed's Basic Science Trivia Quiz -- have a chuckle! Rudolf Virchow on Pathology Education -- humor Curriculum Position Paper -- humor The Pathology Blues  Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
|


 Musculoskeletal
Musculoskeletal
 "Why I Support Amateur Boxing"
"Why I Support Amateur Boxing"
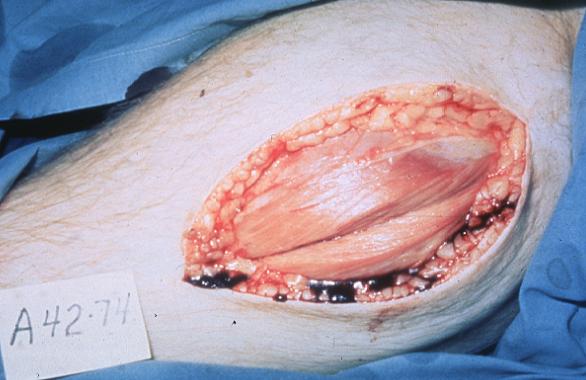 Duchenne's muscular dystrophy
Duchenne's muscular dystrophy