Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com
No texting or chat messages, please. Ordinary e-mails are welcome.

|
|
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected. No texting or chat messages, please. Ordinary e-mails are welcome.
 I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with peoples' health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:

My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!

![]()
![]()
|
|
|
|
|
|
|
|
|
|
|
|
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- Bones / Joints / Soft Tissue Tumors
Lectures follow Textbook
QUIZBANK: Bone & joint #'s 57-106
INTRODUCTION
Most patients with arthritis do not know which type they have (Mo. Med. 87: 145, 1990), and, appropriately, most cases of joint disease never get examined by a pathologist. Yet joint problems are the #1 recognized cause of occupational disability, and cause suffering comparable in prevalence and severity (though not in kind) to alcoholism and major mental illness.
This unit includes a major systemic disease (rheumatoid arthritis) and several important single-organ problems. You have completed the LEARNING OBJECTIVES when you know the handout at recall level, and have examined the photos in "Big Robbins" or your own favorite pathology text.
Several of the major diseases (rheumatoid arthritis, juvenile idiopathic arthritis, the enthesopathies) feature inflammation in the absence of obvious autoimmunity. An evolving word, AUTOINFLAMMATORY, may come to describe this category of disease, in which some sort of vicious cycle in the chaotic immune system leads to mysterious illness. Although most folks today still reserve "autoinflammatory" for entities like familial mediterranean fever, the usage may someday encompass these diseases, as well as psoriasis, ulcerative colitis, Crohn's regional enteritis, and even alcoholic liver disease (which mysteriously spares the large majority of heavy drinkers).
"Joint diseases" involve the diarthrodial (hinge, synovial) joints. (Rule: Disease does not affect synarthrosis, i.e., non-moving, joints like skull sutures or the pubic symphysis). Don't forget the major autoimmune diseases and fibromyalgia syndrome in evaluating musculoskeletal or joint pain.
Anatomy:
You remember that type A synovial lining cells are phagocytes, capable of elaborating macrophage cytokines. Type B "synoviocytes" make collagen, proteoglycans, and are now established as the source of hyaluronic acid. There is no basement membrane under this quasi-epithelium, so water passes freely in and out of the synovial fluid.
"Narrowing of the articular space" on x-ray usually means the cartilage is thinned or gone.
* Articular cartilage has four layers (superficial, intermediate, deep, and calcified) that are usually easy to spot unless there is advanced damage / osteoarthritis. Ask a biochemist to review the fascinating molecular biology of cartilage. Collagen keeps the masses of aggrecan proteoglycan compressed like rubber balls bound tight in a fishnet to keep everything springy. Everything is anchored tight to the chondrocytes. Matrix metalloproteinases such as stromelysin 1 tear the matrix down in response to a variety of stimuli, etc., etc.
Many major systemic diseases affect joints.
These include amyloidosis, gout, lupus, Lyme
disease![]() ,
hemochromatosis, Wilson's copper overload,
hemophilia (or other causes of bleeding into a joint -- hemosiderotic arthropathy), hepatitis C arthropathy,
HIV, inflammatory
bowel disease (most forms and also post-ileal-bypass), ochronosis ("alkaptonuria"; "I can't clean
your diaper"; cartilages are black due to a defect in metabolism tyrosine / phenylalanine breakdown), reactive arthritis, rheumatic fever, sarcoid, scleroderma, sickle cell disease,
syphilis
,
hemochromatosis, Wilson's copper overload,
hemophilia (or other causes of bleeding into a joint -- hemosiderotic arthropathy), hepatitis C arthropathy,
HIV, inflammatory
bowel disease (most forms and also post-ileal-bypass), ochronosis ("alkaptonuria"; "I can't clean
your diaper"; cartilages are black due to a defect in metabolism tyrosine / phenylalanine breakdown), reactive arthritis, rheumatic fever, sarcoid, scleroderma, sickle cell disease,
syphilis![]() , and various
viremias.
, and various
viremias.
{49499} ochronosis ("alkaptonuria"), femoral head
You remember that alkaptonuria makes cartilage turn black and flake, causing bad osteoarthritis by early middle age. The pigment, of course, is homogentisic acid, a phenylalanine-tyrosine metabolite.
Also remember the various causes of clubbing (and its severe counterpart seen in non-oat-cell lung cancer, "hypertrophic osteoarthropathy") and neuropathic joint disease ("Charcot's joints").
ANKYLOSIS of a joint is scarring that is sufficient to prevent movement in that joint.
"OSTEOARTHRITIS" ("osteoarthrosis", "degenerative joint disease"; Lancet 350: 503, 1997; Med. Clin. N.A. 81: 85, 122, 1997; Ann. Int. Med. 133: 635, 2000; Postgrad. Med. 114: 11, 2003; Lancet 365: 965, 2005; Clin. Orth. 427-S, 2004; Med. Clin. N.A. 93: 1, 2009 from KU).
A very common, slowly progressive, initially-noninflammatory process of unknown cause, normally occurring later in life.
Regardless of cause, the joint cartilage alters chemically and exhibits cracks perpendicular to the surface. Eventually, it becomes thinner.
* One animal model is the collagen VI-deficient mouse (Arth. Rheum. 60: 772, 2009).
In addition, the nearby perichondrium is activated, producing knobs off the side of the joint, and the synovium may undergo some thickening or transformation into scar, cartilage, and/or fat.
Most osteoarthritis fortunately never becomes symptomatic. When it does, victims experience the slow onset of stiffness, pain, minor deformity and limitation of motion without heat or effusion.
Most often involved are the great weight-bearing joints of spine, hips, and knees.
Especially troublesome is lipping in the cervical and lumbar spine ("osteophytes"), which can impinge on nerve roots of the spinal foramina.
At least some of the pain must be from the re-sprouting of damaged nerves in the joints -- demonstrated by the partial effectiveness of tanezumab, a nerve growth factor inhibitor, in helping the pain of osteoarthritic knees (NEJM 363: 1521, 2010).
For some reason, the phalangeal-metacarpal joint of the thumb, distal interphalangeal joints (spurs here are called "Heberden's nodes"), and TMJ are also commonly involved. (Needless to say, these are not "heavy weight-bearing joints".)
* Medical history buffs: This is the same Dr. Heberden who distinguished chickenpox from
smallpox![]() ,
described angina pectoris, and described night blindness.
,
described angina pectoris, and described night blindness.
"Bouchard's nodes" are similar, but on the proximal interphalangeal joints.
* The osteoarthritis at the base of the thumb usually occurs in women, usually at menopause. A basic scientist presents an elaborate hypothesis as to why this should be so: Clin. Ortho. Rel. Res. 438: 266, 2005.
* Wearing high-heeled shoes as a likely cause of knee osteoarthritis: Lancet 351: 1399, 1998. Makes sense.
The wrists, elbows and shoulders are generally spared.
PRIMARY OSTEOARTHRITIS is the common "arthritis" that affects most older people.
This is supposedly due to "wear-and-tear" (it's more common in big people, especially in the overweight; mechanical ideas revisited Rheumatology 45: 146, 2006; Clin. Orth. 427: S-96, 2004) and/or metabolic changes in cartilage (the bewildering array in "Big Robbins" is only the beginning, but they cannot all be primary.)
The old notion that chondrocytes don't ordinarily divide is clearly not true; chondrocytes of the elderly show plenty of evidence of cell senescence, including greatly shortened telomeres and very altered metabolism, and this probably has something to do with osteoarthritis (J. Bone Joint Surg. 85-A (S2): 106, 2003). Correlating aging, joint loading, and osteoarthritis using cell cultures subjected to a variety of conditions: CLin. Ortho. Rel. Res. 427-s: S-96, 2004.
Further, in osteoarthritis, we may see heroic chondrocytes that have undergone hypertrophy, become binucleate, etc., etc. in an ultimately-doomed attempt to to keep the cartilage going.
SECONDARY OSTEOARTHRITIS has an identifiable congenital or acquired predisposing factor (i.e., football knee, dancers, power drill operators, heavy people who do a lot of kneeling or squatting (Arth. Rheum. 43: 1443, 2000), congenital hip malformation, hemochromatosis, deposits, defective type II procollagen gene COL2A1 (Arth. Rheum. 42: 39, 1999; Arth. Rheum. 51: 925, 2004; the many forms Arth. Rheum. 62: 1421, 2010), iron or copper overload, ochronosis/alkaptonuria, acromegaly, and some obscure genetic syndromes. Most famous is post-traumatic osteoarthritis, yet at the level of pathophysiology it is almost entirely mysterious (Clin. Orth. Rel. Res. 423: 7, 2004).
Athletes probably do not have more osteoarthritis than others (for example, Am. J. Med. 88: 452, 1990), but there are many variables. Basketball players get osteoarthritis in the knees. Baseball pitchers get osteoarthritis in the shoulders and elbows. Soccer players who take trauma to the knees have a very high prevalence of osteoarthritis in later years, but longtime runners do not. And so forth. The key seems to be loading plus twisting the joint, which would seem to do the most damage to the cartilage.
Burned-out Lyme disease![]() looks anatomically like osteoarthritis. (During
the active phase, Lyme disease synovium looks like rheumatoid arthritis.)
looks anatomically like osteoarthritis. (During
the active phase, Lyme disease synovium looks like rheumatoid arthritis.)
* Today, some pathologists and clinicians are talking about subtypes of osteoarthritis. Maybe this will lead to further clarification, but since this isn't really a pathologist's disease and tissue samples are rare, expect ongoing confusion. Here's one classificaiton:
| KASHIN-BECK DISEASE is an ancient, endemic, deforming disease of bones and joints seen today only in Tibet and some of the other remoter areas of Mainland China. (Formerly it was seen in North Korea, Mongolia, and Siberia but has vanished as nutrition has improved.) It begins in childhood and cripples up to 90% of people in some of the poorest communities. The underlying lesion is evidently non-formation of the little arteries that should supply the cartilage plates (Int. Ortho. 25: 151, 2001), explaining both the arthritis and the dwarfing of the limbs. The cartilage itself undergoes necrosis (J. Bone Min. Metab. 24: 319, 2006). The cause is almost certainly selenium deficiency plus vitamin E deficiency (Clin. Rheum 16: 441, 1997; NEJM 339: 1112, 1998 -- Beijing finally completed a study and found supplementing helps keep their Kashin-Beck region kids from getting crippled: Osteoarthriis & Cartilage 17: 144, 2009) and maybe iodine deficiency (NEJM 339: 1156, 1998; selenium-plus-iodine animal model Osteoarth. Cart. 15: 1171, 2007) coupled with fulvic acid in the drinking water. (The fulvic acid comes from rotting organic material; it poisons procollagen type II processing Eur. J. Biochem. 202: 1141, 1991; J. Tox. 35: 79, 1992; Am. J. Clin. Nut. 57(S2): 259S, 1993; Int. Ortho. 25: 188, 2001). Animal model: Biochem. J. 289: 829, 1993. Histopathology Virch. Arch. A. 423: 483, 1993. Conference in Beijing Br. Med. J. 318; 485, 1999. It's still part of life in parts of China: J. Rheum. 35: 696, 2008; Tibet Am. J. Clin. Nutr. 78: 137, 2003 (as the rich in China get richer, the Belgians have to come in to run tests and offer selenium and iodine supplements on China's poor kids). The "official" line from China today (2010) seems to be that it's a genetic disease... uh. | 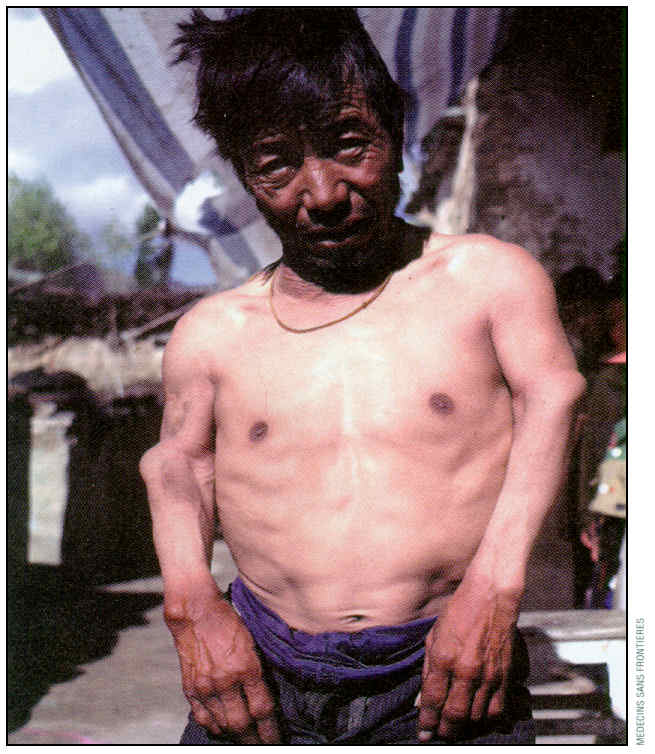 Kashin-Beck |
Regardless of whether osteoarthritis is "primary" or "secondary", the pathologist sees characteristic changes:
* A group in Germany finds that in a pig model, osteoarthritic joints can have their cartilage fully resurfaced by biotech-modified cells; alas, the new surface falls off after about six months! But stay tuned (Arth. Rheum. 58: 475, 2008).
A variety of novel therapies are on the horizon, from injecting joints with the glucoprotein lubricin (Arth. Rheum. 60: 840, 2009) to injecting hyaluronan (Rheumatology 47: 1172, 2008). Since nothing's available that alters what's known about the interplay of damage, healing, cartilage, and subchondral bone, your lecturer doubts any of these will be hugely effective. More encouraging: A small molecule "kartogenin" that encourages endogenous stemcells to differentiate as full-fledged matrix-producing chondrocytes (NEJM 366: 2522, 2012).
CHARCOT'S NEUROPATHIC CHANGE ("neurogenic arthropathy"; "neuropathic joint disease") is a marked deformity of one or more joints in an area where sensation has been lost (update Lancet 366: 2058, 2005).
The old explanation that it represents the result of repeated injury obviously doesn't make sense, and there are cases in which it has almost overnight. There is a mechanism awaiting discovery -- it will involve unknown interactions between bone and nerve. (Osteopathic students take note!)
{10946} spurred spine
{24637} spur, histology
{24638} eburnation
{24639} "cyst" formation in articular bone
{24640} joint mouse
{40180} femoral head, eroded cartilage
{45612} x-ray, showing narrowed joint spaces
|
|
|
|
|
|
RHEUMATOID ARTHRITIS ("RA"; poem NEJM 320: 674, 1989; Lancet 358: 903, 2001; Lancet 373: 659, 2009; Lancet 376: 1094, 2010; molecules NEJM 365: 2205, 2011) |
 Renoir |
With great success researchers have dismantled the pathogenic subunits of RA, adding gene to gene, molecule to molecule, and pathway to pathway in an ever more complex scheme of dysfunction. The complexity of the emerging disease model leaves us speechless.
-- J. Clin. Inv. 116: 869, 2006; from Emory
A common, usually chronic, systemic, dread inflammatory disease (* probably a group of diseases) of unknown etiology. Its outstanding feature is progressive, symmetrical synovitis, with pain and morning stiffness, and which may lead to deformity and destruction of the joints.
Up to 3% of women and 1% of men worldwide will be affected; most cases arise in young or middle-aged adults. The American Indians have a very high prevalence of rheumatoid arthritis. Why women get more rheumatoid arthritis is mysterious; no doubt it has something to do with women's immune system being more powerful than men's. Going on the oral contraceptive pill has been said to help RA, and estrogen actually relieves some animal models. Smoking greatly increases the risk (Arth. Rheum. 54: 38, 2006 -- links to citrullination of proteins).
{25016} rheumatoid arthritis, ulnar deviation
{25017} rheumatoid arthritis, ulnar deviation
{38225} rheumatoid arthritis, hand
{45602} rheumatoid arthritis, x-ray
{45648} rheumatoid arthritis, foot
|
|
|
|
|
|
|
|
The genes behinds of rheumatoid arthritis are just now starting to be worked out. The only genes presently well-linked are some alleles of HLA-DRB1 (a component of the HLA system) and (weaker) an obscure tyrosine phosphatase (Rheumatology 47: 399, 2008). It's been known for about a decade that, whatever number is assigned the actual high-risk tissue-type, they have a common five-amino-acid epitope (HLA-DRB1 SHARED EPITOPE: Arth. Rheum. 42: 2698, 1999; Arth. Rheum. 43: 753, 2000; * QKRAA/QRRAA/RRRAA). There are also possible links to the TNF locus (Arth. Rheum. 54: 1105, 2006) and the gamma-interferon locus (Lancet 356: 783, 2000). The identical twin of a RA patient has only about a 30% chance of getting the disease.
An acute ("exudative", i.e., lots of neutrophils and fibrin, hyperplastic synovial cells, and obviously destructive) and chronic inflammatory synovitis leads to proliferation of a vascular connective tissue in the synovium, which later fills with polys, T-cells, and plasma cells ("pannus"). Venules assume the form and function (* "high endothelial", i.e., very permeable to lymphocytes) seen in lymphoid tissue. You won't see pus. On arthroscopy, pannus looks like a sea anemone.
Pannus spreads over and erodes the articular cartilage and even bone leading to fibrosis of the joint. Fibrin may produce "rice grains" floating in the synovial fluid.
{49503} pannus, gross
{49504} pannus, gross
{46391} pannus, gross, up close
{24636} pannus, micro, eroding bone
{10313} pannus, micro, eroding bone
{19415} pannus, showing lymphocytes
{19418} pannus, showing lymphocytes
Obviously, rheumatoid arthritis is immune-mediated, and on the evidence, the "driver" (J. Imm. 183: 191, 2009) is interleukin 17, the marker for Th17 cells. Big review Clin. Immuno. 132: 295, 2009.
All about IL-17 and T-17 cells, now the principal suspects in rheumatoid arthritis and some other immune diseases: NEJM 361: 888, 2009; J. Imm. 184: 3233, 2010; Blood 115: 335, 2010. Update on IL-17, including its being chemotactic for monocytes/macrophages (J. Imm. 182: 3884, 2009). Not surprisingly, an anti-interleukin 17 monoclonal antibody seems to help rheumatoid arthriits (Arth. Rheum. 62, 929, 2010) -- watch this one.
The macrophages (not lymphocytes) in turn seem to produce other mediators that cause the problems. Mediators of inflammation that seem strongly involved in rheumatoid arthritis are macrophage-derived: IL-1, IL-6 (Br. J. Rheum. 34: 321, 1995), interleukin-8 (J. Lab. Cln. Med. 123: 183, 1994), leukotriene B4, complement components, and α-TNF (it abounds in rheumatoid fluids). Very likely the type A synovial cells are among the "macrophages" that elaborate these. The cytokines summon the polys and cause other harmful things to happen.
Interleukin 1 (and more recently, α-TNF) have been shown to stimulate production of collagenase and prostaglandin E2 in rheumatoid joints. Another usual suspect is interleukin 6, produced by the synoviocytes themselves (Am. J. Path. 152: 821, 1998). All of these cause havoc.
Substance P, released from nerve terminals in joints, is also a perennial suspect (update Br. J. Pharm. 144: 1059, 2005). This is in keeping with observations that emotional stress triggers flare-ups, and that joints paralyzed by strokes are spared the effects of rheumatoid arthritis. Relate all this to the mouse model of scrambled neural circuitry, and the atypical depression of rheumatoid arthritis patients: JAMA 267: 910, 1992.
* Autoantibodies against type II collagen are often reported in rheumatoid arthritis. Whether these are primary, or the result of secondary sensitization to damaged cartilage in an area already overflowing with B-cells, is unclear (Arthr. Rheum. 42: 2569, 1999).
Fibroblasts in rheumatoid arthritis synovium ("rheumatoid arthritis synovial fibroblasts", RASFs) adhere inappropriately to cartilage and produce enzymes that degrade it.
Food hypersensitivity is related anecdotally to some cases of rheumatoid arthritis, and some of the evidence is impressive. Patients may experiment with elimination diets.
Despite the fact that the problem seems to begin with T-cells rather than B-cells, two autoantibodies are quite common in the disease.
RHEUMATOID FACTOR, present in most RA patients, is polyclonal antibody (mostly IgM, often IgA) against the Fc portion of IgG. When present, the patient is said to be "seropositive"; otherwise, "seronegative." Its presence means the disease is more likely to be familial, there is more likely to be vasculitis, there are more likely to be rheumatoid nodules, and there is more likely to be eye involvement. Contrary to older teaching, higher titers also suggest greater disease severity. See Arth. Rheum. 50: 2113, 2004, lots more.
ANTI-CCP (antibodies against anticyclic citrullinated peptide) is the up-and-coming test for rheumatoid arthritis, with claims of 80% sensitivity and 99% specificity. The antibodies turn positive a few years before disease onset, as do rheumatoid factors (Arth. Rheum. 48: 2741, 2003; J. Imm. 175: 5575, 2005). Several commercial assays all seem to work okay -- Rheumatology 49: 450, 2010.
The presence of anti-CCP predicts more severe disease (by now well-established: Arth. Rheum. 56: 2929, 2008). Anti-CCP-negative rheumatoid arthritis may well be a different, milder disease, as the cells in the synovium are quite different (Arth. Rheum. 58: 53, 2008).
As you've surely guessed, synovium in health and disease does contain citrullinated proteins of various sorts (Arth. Rheum. 54: 3809, 2006) -- not much is known about them.
* Of course, there are subclasses. One is "anti-MCV / anti mutated citrullnated vimentin".
Small joints are most often affected, especially the proximal interphalangeal joints (swan-neck deformity, boutonniere deformity, sometimes ankylosis, more often subluxation), metacarpophalangeal joints (ulnar deviation), wrists, knees, ankles. Tendons may rupture, especially those that extend the last two fingers.
Whatever the cause, central to today's thinking about rheumatoid arthritis is the understanding that the irreversible destruction of the joints begins with the first symptoms, and is cumulative and progressive. Hence the emphasis on disease-modifying medications (methotrexate, many others from various classes) early-on, rather than just anti-inflammatories. See below.
|
{24635} rheumatoid arthritis, damaged joint
|

|
There's still debate as to whether rheumatoid joints really are stiffer in wet weather (Scand. J. Rheum. 15: 27, 1986 vs Proc. Nat. Acad. Sci. 93: 2895, 1996; J. Rheum 29: 335, 2002).
Rheumatoid subluxation of the cervical spine is a surgical emergency when the spinal cord is compressed.
"Geodes" are subchondral pseudocysts, in which the bone degenerates and fills with debris, as in one of the familiar hollow rocks with crystals inside. Usually in rheumatoid arthritis; you can see them in osteoarthritis, aseptic / avascular necrosis, gout or pseudogout too.
{30286} rheumatoid disease of axis
{30288} rheumatoid disease of axis
The rheumatoid arthritis patient has a systemic disease and often many other problems:
Patients may develop splenomegaly (when this causes neutropenia / pancytopenia, this is FELTY'S SYNDROME: Update J. Rheum. 32: 20, 2005 -- now thankfully quite rare Dig. Dis. Sci. 56: 95, 2011), ANEMIA OF CHRONIC DISEASE, generalized LYMPHADENOPATHY (J. Clin. Path. 43: 106, 1990), and/or MYOPATHY. Mild FEVER and severe MALAISE are common. AMYLOIDOSIS occurs in around 15%, especially the more severe cases (Br. J. Rheum. 35: 44, 1996). THese effects must be cytokine-mediated; for years IL-1 was the principal suspect, but stay tuned.
RHEUMATOID LUNG -- fibrosis of the alveolar septa, which make them impermeable to oxygen and decreases lung compliance -- occurs in around a quarter of these patients. RA patients must stop smoking. Fibrous tissue may also selectively obliterate the bronchioles and small vessels. Update, emphasizing speculative mechanisms: Am. J. Med. Sci. 321: 83, 2001. Acute exacerbations are unexplained but deadly: Chest 132: 214, 2007.
RHEUMATOID NODULES occur in maybe 20% of patients with rheumatoid arthritis (and many patients with rheumatic fever, or with neither).
These consist of an acellular center of eosinophilic material ("fibrinoid", as before a mix of plasma proteins) surrounded by palisaded histiocytes and other cells, maybe with a rim of granulation tissue.
They may occur nearly anywhere; most often about extensor surfaces, sometimes the pericardium, aortic valve (thankfully rare), lung parenchyma (coal miners -- that's Caplan's syndrome, part of the "black lung" complex.)
* It's generally agreed that patients with rheumatoid arthritis are at extra risk for coronary artery atherosclerosis, probably from inflammatory damage to the intima. See Arth. Rheum. 61: 1580, 2009.
{12473} rheumatoid nodule, patient
{09000} rheumatoid nodule, histology
{08999} rheumatoid nodule, histology
OSTEOPOROSIS develops around affected joints. It's not just disuse -- the process seems to melt bone.
Rheumatoid VASCULITIS (type III immune injury, no surprise in a disease in which antibodies can be directed against themselves) can and do cause MI, stroke, gangrene, finger and leg ulcers, Raynaud's, etc. Check these patients for CRYOGLOBULINS.
SJOGREN'S SYNDROME can develop (* 15%).
PLEURISY (painful inflammation of the pleural surfaces) can develop and produce effusions that compress the lungs. PERICARDITIS is less common.
* The older "treatment pyramid" had as its base aspirin or non-steroidal anti-inflammatory drugs, muscle-strengthening, and rest.
Immunosuppression used to be reserved for resistant cases, but there was never any shortage of such patients. Today, disease-modifying treatments are started much earlier. Methods include glucocorticoids, antimetabolites such as azathioprine, methotrexate (today's most important agent), cyclophosphamide, cyclosporine, others. Also tried are total lymphoid radiation, gamma interferon, anti-CD4 monoclonal antibody and more. Strong medicine -- but certainly worth trying before your RA patient commits suicide.
The 1990's saw oral administration of altered type II collagen to "tolerize" the T-cells (however that works, and it seems to, at least for a minority of patients): Science 261: 1727, 1993; Arth. Rheum. 39: 41, 1996); some small studies with variable results since.
Omega-3's (fish oil) probably help in controlling symptoms of rheumatoid arthritis (Arthr. Rheum. 37: 824, 1994) by blocking production of leukotriene B4 and interleukin 1.
Vitamin E fails a fifteen-year study in primary prevention of rheumatoid arthritis in women: Arth. Rheum. 59: 1589, 2008.
The BIG news in rheumatoid arthritis is the spectacular success of the biotech antibodies products that alter the function of various molecules involved in rheumatoid arthritis.
Rituximab (B-cell depleter): NEJM 350: 2546 & 2572, 2004 -- it seems to work by reducing Th17 cell response by some B-cell-mediated mechanism (Arth. Rhem. 63: 1507, 2011). Anakinra, the interleukin-1 receptor antagonist: Rheum. Dis. Clin. N.A. 30: 365, 2004. Abatacept (Orencia): T-cell co-stimulation modulator, a fusion protein that stops T-cells from talking to B-cells. Ann. Int. Med. 144: 865, 2006. Tocilizumab (interleukin-6 receptor inhibitor) is now in use clinically Arth. Rheum. 63: 1255, 2011; Lancet 381: 1541, 2013.
* Talk about a "novel therapy".... the principal component of cryptococcus capsular polysaccharide, glucuronoxylomannan, reduces STAT3 signalling (the main control in IL-17), and hence RORgammat synthesis, and hence IL-17 production (J. Immuno. 183: 191, 2009).
The rate of malignant lymphomas is somewhat increased (maybe doubled) in rheumatoid arthritis patients; contrary to older concerns, this does not seem to be due to therapy, but to some intrinsic property of the disease (i.e., all the divisions of those lymphocytes). Update Arth. Rheum. 50: 1740, 2004.
Manipulation failed in one study when applied for rheumatoid arthritis: J. Musculoskel. Med., June 1990. In evaluating any therapeutic claim you may hear for rheumatoid arthritis, remember that it is a disease of exacerbations and remissions, many cases just go away, and only a minority lead to profound deformity and disability ("arthritis mutilans"). Arthritis quackery was a huge money-maker during the era when scientific medicine had little to offer. The copper bracelet is a harmless, useless folk charm.
JUVENILE IDIOPATHIC ARTHRITIS ("juvenile rheumatoid arthritis"; "Still's disease"): Review Ped. Clin. N.A. 52: 413, 2005; Lancet 369: 767, 2007; Lancet 377: 2138, 2011.
Apparent rheumatoid arthritis in one or more joints beginning under age 16 (peak incidence 1-3 years). It has always been clear that this is several different diseases of various etiology, and the molecular studies (too arcane for medical school undergraduates!) have demonstrated beyond any doubt.
A febrile prodrome for weeks or months, big lymph nodes and liver, pleuritis, pericarditis, iridocyclitis, and/or skin rash may appear.
Rheumatoid factor may be present but is more often absent. ANA is often positive. Again -- don't worry about the subtypes now; specialize tests will guide treatment. Many cases remit.
The immunopathology remains poorly understood. Some forms feature an anemia which is quite severe, more so than the "anemia of chronic inflammation" familiar from rheumatoid arthritis.
It's now emerging that IL-17+ T-cells are abundant in the synovium of these patients, especially with the more severe variants (Arth. Rheum. 58: 875, 2008) as in rheumatoid arthritis; others do not have this.
Despite the obvious differences between Still's disease and classical rheumatoid arthritis, the anatomic joint changes appear to be the same.
There is often talk of an infectious agent as the cause of JRA/JIA, but despite various reports, there's still nothing solid.
* Autologous stemcell transplantation for cure of refractory JRA/JIA: Lancet 353: 550, 1999.
Remember parvo B19![]() as a cause of sudden horrendous multi-joint disease
in anybody. It may hang on for a long, long time.
as a cause of sudden horrendous multi-joint disease
in anybody. It may hang on for a long, long time.
Some of the alphaviruses produce a mild arthritis in humans that can sometimes be severe and enduring (for example, Chikungunya arthritogenic alphavirus, of tropical Africa and Asia: J. Immuno. 184: 5914, 2010); J. Inf. Dis. 203: 149, 2011; now a major emergent disease Lancet 379: 662, 2012; Lancet 379: 662, 2013; it's now on southern Europe and is surely on its way to the USA.
Of course, Lyme disease![]() is in the "differential" of any kid with "JRA/JIA".
is in the "differential" of any kid with "JRA/JIA".
PALINDROMIC RHEUMATISM is a curious illness in which one or two joints at a time get very painful and inflamed, subsiding in a few hours or days, followed by others. The disease is usually self-cures without damage, but may be the prodrome to rheumatoid arthritis or lupus.
"THE REACTIVE ENTHESOPATHIES" (seronegative spondyloarthropathies, HLA-B27 family; these are NOT "variants of rheumatoid arthritis")
This is a curious family of common, overlapping illnesses that include ankylosing spondylitis (Lancet 369: 1379, 2007; also known as Marie-Strumpell disease, "bamboo spine", "poker-back"), reactive arthritis from urethritis ("Reiter's), enteropathic arthropathy (shigella, salmonella, campylobacter, yersinia, ulcerative colitis / Crohn's, and the joint disease of psoriasis (big review Postgrad. Med. 97(4): 97, April 1995). All are more common and more severe in men.
{46390} ankylosing spondylitis
{49505} ankylosing spondylitis
{49506} ankylosing spondylitis
An "enthesis" is the point at which a ligament attaches to bone. The axial entheses are involved. Joints do not erode, but ankylose (fuse solid), with bone actually connecting to bone (even marrow to marrow) around joints and disks.
Remember they are all much more common in people with HLA-B27 (though only about 5% with the allele get it). This now seems to be generalizable to all populations; frequency of HLA-B27 and ankylosing spondylitis in a population correlates; the allele and disease are most common in the Inuit (Eskimos -- half of them carry HLA-B27). Rheumatoid factor is not present and synovial membranes are usually not inflamed.
It's now generally agreed that these are the result of T-cell sensitization to some component of the enthesis. Right now, the principal suspect is aggrecan (Rheumatology 42: 846, 2003, Ann. Rheum. Dis. 62: 561, 2003, Ann. Rheum. Dis. 64: 722, 2005; others).
The pathology mostly involves ligamentous attachments, with a mix of acute and chronic inflammation and scarring. There's likely also to be some inflammation in the fingers toes, clinically and/or on imaging. You remember the relationship to reactive arthritis (formerly "Reiter's), which shares some of the back morphology and the early type of back pain; you won't confuse the two.
Doctors -- heads up! Five percent of your severe low-back-pain patients, and a higher percent of those who can't relate it to strain or injury, have ankylosing spondylitis. If you diagnose it early (i.e., before the classic stuff is obvious), you can use the new biologicals to control it. Here's your tip-offs:
Infliximab and etanercept were used off-label for ankylosing spondylitis for several years and obviously worked. The FDA has now approved this use. Adalimumab (the third anti-TNF-alpha agent to be approved in the US) greatly increases quality of life: Arth. Rheum. 57: 1050, 2007; Rheumatology 48: 551, 2009.
Ustekinumab, the interleukin 12/23 blocker, for psoriatic arthritis: Lancet 373: 633, 2009 (skin and joints both helped). Secukinumab, an interleukin 17A inhibitor, for psoriatic arthritis: NEJM 373: 13329, 2015. Brodalumab, the antibody against the interleukin 17A receptor, for psoriatic arthritis: NEJM 373: 1318, 2015.
REACTIVE ARTHRITIS is a syndrome that follows a bacterial infection
that seems to trigger a strange immune response. It features
arthritis, eye problems, and a horny rash on the glans, trunk, and especially
palms and soles, all following an episode of urethritis or infectious
gastroenteritis (* "Can't see, can't pee, can't climb a tree, can't go
out with me!"). Most patients are men; most are HLA-B27 positive.
Chlamydia![]() have been reported in the pannus: Arthr. Rheum. 31: 937, 1988; J. Clin. Path. 51: 803, 1998;
obviously most of these people do not get a biopsy. The
symptoms come and go, and generally vanish for good after a few months. This disease is not rare,
and is managed symptomatically (Am. Fam. Phys. 60: 499, 1999)
or (if it's chlamydia) six months on antibiotics (Arth. Rheum. 62: 1298, 2010).
have been reported in the pannus: Arthr. Rheum. 31: 937, 1988; J. Clin. Path. 51: 803, 1998;
obviously most of these people do not get a biopsy. The
symptoms come and go, and generally vanish for good after a few months. This disease is not rare,
and is managed symptomatically (Am. Fam. Phys. 60: 499, 1999)
or (if it's chlamydia) six months on antibiotics (Arth. Rheum. 62: 1298, 2010).
{12289} Reactive arthritis, scaly rash
{12290} Reactive arthritis, scaly rash
Spondylitis patients tend to get better by themselves, especially after the spine is no longer mobile. And remember that some people diagnosed with "ankylosing spondylitis" may actually have reactive arthritis or anything else in this section.
POLYMYALGIA RHEUMATICA is a poorly-understood, very underdiagnosed, very common pain syndrome without any known anatomic correlate or joint findings, usually occurring in folks over age 50, with morning stiffness and pain especially in the neck, shoulders, and/or pelvic girdle. The sed rate and CRP are reliably elevated and the response to a low dose of a glucocorticoid is dramatic. It runs with the more ominous temporal arteritis. See Lancet 381: 63, 2013.
LOW BACK PAIN (remember there's also "neck pain"). Review Br. Med. J. 310: 929, 1995; update Lancet 369: 726, 2007. I strongly recommend the Lancet 2007 article, and not just because it urges practitioners to consider referring patients for manipulation.
This ubiquitous clinical problem has baffled the scientific medical profession until recently:
(1) Imaginary etiologies (notably "muscle spasm") are routinely invoked to explain it, resulting in a whole class of drugs ("muscle relaxants") that are used very questionably. (I hope you enjoy reading "The Myth of Skeletal Muscle Spasm", Am. J. Phys. Med. Rehab. 68: 1, 1989, as much as I did.)
(2) Bulges and protrusions (but not extrusions) seen on MRI scans were considered etiologic, until it turned out that folks without back pain have indistinguishable "pathology" (NEJM 331: 69, 1994).
(3) Anecdotal evidence of better results from treatment through "systems of alternative medicine" (osteopathy, chiropractic), which treat back pain using empirical techniques. See West. J. Med. 150: 351, 1989. This has found recent support in a few pretty good controlled studies: Br. Med. J. 300: 1431, 1990; Lancet, July 28, 1990, p. 220, others.
(4) Discovery by the medical profession of such common-sense processes as FACET SYNDROME (update Anesthesiology 106: 591, 2007), which is now recognized as among the most common cause of back pain without sciatica; and little TEARS IN THE ANNULUS FIBROSUS (which is innervated and doesn't heal well; Br. Med. J. 312: 169, 1996)
Risk factors for low back pain are tall stature, overweight, large breast size, slouching, lack of
physical conditioning,
cigaret![]() smoking (Lancet 1: 1305, 1989), and drunkenness. Truck drivers and
nurses have more than their share of back troubles.
smoking (Lancet 1: 1305, 1989), and drunkenness. Truck drivers and
nurses have more than their share of back troubles.
Mechanical problems that give rise to low back pain are only now being elucidated.
It has been known for centuries that the nucleus pulposus has dried up and the annulus has cracked in most discs by age 60. These cause a variety of problems (Hosp. Pract. 24: 135, Sept. 1989).
When a nucleus pulposus herniates through the annulus and impinges on a nerve root, the pain can be severe. (You'll learn about the "straight leg raising test" and other techniques in clinic).
In "facet syndrome", we think that the posterior inter-laminar facet joints sublux as a result of disc space narrowing. Patients typically report sudden onset on bending or twisting, have negative straight leg raising tests, and have relief when a local anesthetic is injected into the joint.
Another plausible-sounding theory of the origin of this kind of pain is herniation of a bit of synovium into the space around the nerve -- it's easy to see how manipulation could relieve this problem immediately. Stay tuned.
* Yet another idea -- nerves growing deeper than their usual stopping-point in the outer third of the annulus fibrosus. Lancet 350: 178, 1997.
Magnetic resonance imaging is elucidating the more subtle mechanical problems that have previously eluded radiologists: South. Med. J. 81: 1487, 1988.
Please remember that there are many non-mechanical causes of low back pain. These patient may
have rupturing aortic aneurysms, metastatic cancer, epidural abscesses, Pott's disease (i.e. TB![]() of the
spine), etc., etc.
of the
spine), etc., etc.
* No surprise: Magnetotherapy flops for low back pain JAMA 283: 1322, 2000, JAMA 284: 564, 2000.
{11449} Pott's disease
|
|
"Science is self-correcting". Just as mechanical explanations are finally being figured out, mechanical therapies are finally being appreciated by scientific physicians.
Flaws in previous studies, pro and con: Br. Med. J. 303: 1298, 1991. However, no less a figure than the chief of Harvard's pain clinic has taught physicians (M.D.'s, that is) to perform manipulations Hosp. Pract. 24: 89, March 1989. By now there are dozens of studies of manipulation for low back pain, and most are coming up with "worth considering"; BMJ 329: 1381, 2004 in particular was quite favorable; there are still some concluding "no benefit shown" for this-or-that group. For a subset of low back pain patients, manipulation works at once: Phys. Ther. 89: 1292, 2009 (not blinded; nor were any of the others, really; but this one has dramatic results). The folks at U. of Alberta have proposed the first true-blinded study for OMT: put the patient to sleep with an anesthetic and then either manipulate or don't -- it seems to help some (Arch. Phys. Lab. Med. 90: 366, 2009). I predict that a subgroup will be found (those with some variant of facet syndrome?) for which manipulation will be the treatment of choice. Stay tuned.
The major journals are now publishing positive studies of OMT. A good randomized controlled study of OMT for back pain in later pregnancy showed a good effect (Am. J. Ob. Gyn. 202: 43.e1, 2010). And in the meantime, for pediatric sports injuries generally, Ped. Clin. N.A. 57: 775, 2010 is a peer-reviewed, no-baloney study of OMT's usefulness as an adjunct.
* The website of the
National Association for Chiropractic
Medicine (founded 1984) seems to have vanished.
These "reform chiropractors" were / are
dedicated to upgrading the profession's
scientific and ethical standards.
These reformers called for evidence-based practices,
and met tremendous hostility from ideologues
and
antiscientific practitioners. You'll have a chance to find out about this yourselves.![]() Samuel Homola DC on
Samuel Homola DC on
evidence-based chiropractic --
"An Uncertain Future"
Terms: "radiculopathy", "lumbago" and "sciatica" indicate nerve root involvement, typically with radiating pain. The most common cause, of course, is a bad disc. "Cauda equina syndrome", from compression of the cauda equina by a midline herniated nucleus pulposus, tumor or abscess is a surgical emergency.
Remember there's still malingerers out there. You'll learn a couple of tricks to expose them on rotations.
SUPPURATIVE ARTHRITIS ("septic arthritis", i.e., bacterial infection in a joint; Lancet 375: 846, 2010)
The most common agents are gonococcus, gram positive cocci
(Staph![]() ,
Strep), and gram negative
rods (E. coli, H. 'flu, Pseudomonas; Salmonella in sickle cell disease).
,
Strep), and gram negative
rods (E. coli, H. 'flu, Pseudomonas; Salmonella in sickle cell disease).
These organisms arrive by hematogenous spread.
Suppurative arthritis is uncommon in children (think of H. 'flu or spread from contiguous osteomyelitis).
Bacterial arthritis is usually monarticular and involves large joints. (Gonococcal arthritis often involves a series of joints.)
The cartilage is quickly ruined by hydrolytic enzymes from polys. In bad cases, the joint may end up ankylosed.
|
|
TUBERCULOUS ARTHRITIS follows primary pulmonary infection. It is likely to be bad and chronic, with pannus and ankylosis (Clin. Ortho. 398: 100, 2002.
SYNOVIAL BIOPSY
RELAPSING POLYCHONDRITIS (Ann. Int. Med. 129: 114, 1998)
This is now known to be an autoimmune disease mediated by T-cell sensitization to the collagens in cartilage.
There is a superb mouse model (J. Clin. Invest. 112: 1843, 2003), produced when mice with HLA-DQ8 (the human HLA association) are injected with chicken type II collagen. The mice mount a T-cell reaction against their own collagen II and IX.
In both animals and humans, there are usually antibodies against type II collagen; whether they are pathogenic or secondary to cartilage damage is unknown. As with most autoimmune diseases in humans, it often runs with other autoimmune diseases and responds to immunosuppression. Oral tolerization by feeding type II collagen: Am. J. Med. Sci. 324: 101, 2002.
The onset is sudden and spectacular, but it is a disease of exacerbations and remissions, and it often takes a long time for physicians to consider it.
Symptoms and signs are caused by inflammation of the perichondrium of the ears (very typical), nose (can produce saddle nose) large airways (can be lethal) and joints (painful).
You would rather not biopsy the disease, since cartilage does not heal very well. If you find the characteristic lesion (degenerating cartilage cells under very inflamed perichondrium), you've exacerbated the damage. If not, you'll find only granulation tissue. Make the call on the physical exam.
CALCIUM CRYSTAL DEPOSITION DISEASE:
"Pseudogout" ("chondrocalcinosis") involves deposition of calcium phosphates, usually in the knees. The process is poorly understood, but is very common, especially in older folks.
There is a hereditary form (Gene Arth. Rheum. 48: 2627, 2003). If you have hypercalcemia, hypophosphatemia, or hypomagnesemia, you're at extra risk. By age 80, a majority of people will have some calcium pyrophosphate in the knees. This is especially true if the joints have already been damaged by diabetes, iron overload, or something else.
{14258} pseudogout (or so they tell me...)
{14261} pseudogout (ditto)
![]() "Osteoarthritic" lipping
"Osteoarthritic" lipping
WebPath Tutorial -- comments are down right now
SYNOVIAL SARCOMA
Biphasic (usually, spindle cell and epithelial-like "synovioblast") sarcoma that usually arises in or about Hunter's canal in young adults. (These tumors usually does NOT arise in synovium.)
It metastasizes either by blood or lymphatics. (The latter fact is unusual for sarcomas.)
Prognosis is fair, with 50% ten-year survival.
PIGMENTED VILLINODULAR SYNOVITIS
{09655} pigmented villonodular synovitis, gross
FIBROUS HISTIOCYTOMAS
The cell of origin for all of these curious tumors is the "macrophage acting as a fibroblast". Don't worry about such arcane stuff; leave that to pathologists. We can talk about these here, because several of them affect joints or tendons.
DERMATOFIBROMA ("sclerosing hemangioma"): skin and elsewhere
This is a solitary, hard nodule. The phagocytes contain lipid, making them yellow on cross-section. They also contain hemosiderin, imparting a brown color, and this also causes melanocytic pigmentation of the overlying skin, particularly around the edges, so these appear as brown bumps.
{25592} dermatofibroma, gross
{12203} dermatofibroma, darkly pigmented
{12774} dermatofibroma, gross
{12775} dermatofibroma, gross; this one was quite vascular
{12777} dermatofibroma, gross
{39954} dermatofibroma, section
{24260} dermatofibroma, histology (good spindle-cell histiocytes)
GIANT CELL TUMOR OF TENDON SHEATH ("fingeroma", "xanthofibroma"): quasi-neoplastic benign yellow mass
MALIGNANT FIBROUS HISTIOCYTOMA: the commonest sarcoma, develops deep in limbs or in retroperitoneum.
{21145} malignant fibrous histiocytoma, buttock; you need only recognize this is a deep soft-tissue
cancer (i.e., probably a sarcoma)
{09019} malignant fibrous histiocytoma, histology; you need only recognize this is a spindle-cell
malignancy
{09021} malignant fibrous histiocytoma; you need only recognize this is a malignancy; the cells do
remind me of those in a granuloma
TENDONS AND BURSAE
TENOSYNOVITIS and BURSITIS result from injury (usually mild and repeated). Syndromes includes housemaid's knee (* an occupational hazard of certain monastics as well) and tennis elbow.
{12025} bursitis
OSGOOD-SCHLATTER'S DISEASE is a banal but uncomfortable, very common local ongoing-injury-and-healing lesion involving the anterior tibial tuberosity of athletically-active, rapidly-growing teens. The cause is probably repeated, tiny avulsions of the periosteum from the pull of the quadriceps tendon. See Am. Fam. Phys. 73: 1014, 2006. SEVER'S DISEASE ("calcaneal apophysitis") is a similar overuse syndrome causing pain in the back of the calcaneus.
Not a pathologist's disease either: PLANTAR FASCIITIS is the most common cause of heel pain, and is extremely common in adults, especially those who carry heavy loads at work or just weighing a lot. It hurts worst under the heel, especially on the first step of the day, and there is reduced dorsiflexion of the foot. No one has ever biopsied it, but it must be caused by repetitive microtrauma.
CARPAL TUNNEL SYNDROME: annular fibrosis of the flexor retinaculum, impinging on the median nerve. Very common. Most cases are idiopathic, but remember amyloidosis.
GANGLION CYST: a blob on wrist or fingers, formed by myxoid degeneration of connective tissue. It is neither a "ganglion" nor a "cyst", and it does not communicate with the joint. The home remedy -- smash it with the holy book of your choice -- is about as successful as surgery.
![]() Ganglion cyst, wrist
Ganglion cyst, wrist
Prize photograph
Institute of Medical Illustrators
|
DUPUYTREN'S CONTRACTURE: fibrosis of the palmar aponeurosis with variable/mixed histopathology (chondroid, myxoid, dense scar). It can be a cord or a nodule; in any case, the underlying biology remains completely obscure (Plast. Recon. Surg. 117: 1248, 2006).
* Treating the cord with a collagenase injection followed a day later by mechanically breaking it: NEJM 361: 968, 2009. A similar, often more locally aggressive, lesion can involve the plantar aponeurosis ("plantar fibromatosis"). * Ronald Reagan had a "Dupuytren's" removed while president. "Peter Pan" originator James Barrie had right hand disabled by "tendonitis", maybe Dupuytren's; this became the inspiration for his self-parody as "Captain Hook". (The clock-ticking crocodile who pursues Captain Hook is also allegorical -- the symbol of his premonitions of death.) |  |
{49523} Dupuytren's contracture
The late sequelae of prosthetic joints is only now coming under study. One group suggests that when there is a metal-on-metal joint, tiny particles excite an immune / inflammatory response that is responsible for lysis of nearby bone (J. Bone Joint. Surg. Am. 88: 1183, 2006).
Famous arthritics (Clin. Rheum. 8: 442, 1989): John Madison (rheumatoid arthritis); Renoir (rheumatoid arthritis; his disability influenced his painting style and thus the development of impressionism); Columbus (reactive arthritis? also Arch. Int. Med. 152: 274, 1992).
|
|
|
|
|
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about the pathology of joint disease to consult these standard textbooks.
In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!

| New visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request
| If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |
Teaching Pathology
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |
 |
Click here to
see the author prove you can have fun skydiving without being world-class. Click here to see the author's friend, Dr. Ken Savage, do it right. |


 Musculoskeletal
Musculoskeletal
