Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com
No texting or chat messages, please. Ordinary e-mails are welcome.

|
|
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected. No texting or chat messages, please. Ordinary e-mails are welcome.
 I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with peoples' health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:

My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!

![]()
![]()
Violence is the antithesis of creativity and wholeness. It destroys community and makes brotherhood impossible.
-- Martin Luther King, 1967
We have fed the heart on fantasies,
The heart's grown brutal from the fare;
More substance in our enmities
Than in our love.
-- William Butler Yeats, 1928
"Reflections in Time of Civil War"
No matter what you do, somebody is going to hate you. Look around. See who hates you. Make sure it's the right people.
-- Mothers Against Methamphetamine
Forgiveness is a powerful tool. Use it.
--Nelson Mandela
Razors pain you / Rivers are damp /
Acids stain you / And drugs cause cramp /
Guns aren't lawful / Nooses give /
Gas smells awful / You might as well live.
--Dorothy Parker
Go not in and out at the courts of law, that thy name may not stink.
--Egyptian papyrus, c. 900 B.C.
How many Americans does it take to screw in a light bulb?
Five. One to do it, and four to fill out the environmental impact reports.
--Ed, 1992
The truth is incontrovertible. Malice may attack it. Ignorance may deride it. But in the end -- there it is.
-- Churchill
There is a doctrine whispered in secret that a human being is a prisoner who has no right to open the door and run away.
-- Socrates
Quis, quid, ubi, quidubus auxiliis, cur, quomodo, quando?
What was the crime, who did it, when was it done, and where,
How done, and with what motive, who in the deed did share?
-- from the Latin
Confucius said, "In hearing litigation, I am no different from any other judge. But if you insist on a difference, it is, perhaps, that I try to get the parties not to resort to litigation in the first place."
--Analects XII.13.
People will never stop committing atrocities until they stop believing absurdities.
--Voltaire
Did you hear about the hippie who mixed LSD and prune juice?
He started a whole new movement!
-- Sixties Joke
If you never encounter anything in your community that offends you, then you are not living in a free society.
-- Ms. Kim Campbell, prime minister of Canada
IMOGEN: O, do not make me laugh.
Laughter dissolves too many just resentments,
Pardons too many sins.IACHIMO: And saves the world
A many thousand murders.
-- Shakespeare's Cymbeline (as altered by George Bernard Shaw)
Forensic Pathology Video -- Victorian Institute
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- Environmental / Nutritional
Lectures follow Textbook
|
QUIZBANK Physical injury (all)
|
 "Bringing Out the Dead" |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OBJECTIVES
Describe how the medical examiner's office operates, what deaths must usually be referred there, and how bodies may be identified. Properly complete a death certificate, avoiding the usual pitfalls. Distinguish the various manners and mechanisms of death. Tell how a rural primary care physician called to a crime scene can estimate the time of death.
Describe the most common findings in physical child abuse, and mention the various medical conditions that may simulate it. Distinguish predictable and unpredictable medication side effects. Give the anatomic pathology seen with the common serious drug side-effects. Describe the extent of the illegal drug problem in the US. Recognize needle marks, and describe the internal anatomic pathology and pathophysiology of injectable drug abuse. Give the "two principles" rule for all drug testing that will have medicolegal implications.
Suspect poisoning by thallium, arsenic, mercury, and lead when appropriate. Describe their pathophysiology and distinctive anatomic lesions as applicable. Describe the anatomic pathology and pathophysiology of cocaine use. Give an account of death through excited delirium.
Give a short account of the physiology and health effects of absinthe, cannabis, and the recreational inhalants. Describe the anatomic pathology and pathophysiology, as applicable, of poisoning by paraquat, organophosphates, and dioxin. Describe what we know about the health consequences of caffeine use. Give a full account of what we know about the pathophysiology and anatomic pathology of acute and chronic alcohol abuse, including the quantitative aspects. Describe what happens to people who ingest methanol, isopropanol, and ethylene glycol.
Distinguish abrasions, contusions, lacerations, and the various kinds of sharp-force wounds. Given a weapon or proposed scenario, decide whether it could have produced illustrated pathologic changes. Avoid the common pitfalls. Describe the usual ways in which blunt trauma causes death. Distinguish suffocation, smothering, strangulation, mechanical asphyxia, and choking. Describe the common scenarios, and how you would use pathology to confirm or discredit a scenario. Explain what happens during hanging. Give accounts of the common chemical asphyxiants. Especially, describe what you would see in illness and death due to carbon monoxide toxicity. Describe injuries from extreme heat, and how various kinds of burns do their damage. Describe the pathology of drowning. Explain how pathologists deal with drowning cases. Give a full account of the pathology of blast, decompression, and electrical injuries. Describe how death occurs, and what the pathologist might see, in heat stroke, heat exhaustion, and hypothermia. Explain how a physician might help evaluate the claim of someone seeking asylum and claiming to have been tortured.
Explain how ionizing radiation injures living tissue. Know the various definitions for quantitating radiation and its effects on people. Give the pathology of radiation sickness of varying degrees of severity. Discuss briefly how the nature and impact of war have changed since the beginning of the twentieth century.
Describe the usual situations that lead to homicide.
Describe the usual situations that lead to suicide. After you've reviewed the pathology of violence, talk with your friends about the following often-heard claims. Reasonable people will differ about all of them.
"We are all born good. Criminals are products of their environments." "Violence in the U.S. is largely the result of the entertainment industry." "A physician has a duty to urge people not to keep firearms in their homes."
INTRODUCTION {07130} violent death, don't try these at home Nothing that pertains to human suffering and death is outside the larger domain of human pathology. Knowing what motives underlie most homicides and suicides is as important for a student physician as knowing which special stain helps the lab define a hemangiopericytoma. Most of this unit is about violence. Like most other mammals, when we human beings are HURTING AND CONFUSED at the same time, we have a natural (though lamentable) tendency to lash out against (blame, physically attack) someone else, regardless of the realities of the situation. We've all seen individuals do this, and perhaps we've even done this ourselves.
George Orwell wrote, "We sleep safe in our beds because rough men stand ready in the night to visit violence on those who would do us harm." Like it or not, this is the truth.
Especially since the rise of guerilla warfare, political violence has been directed primarily against civilians. Soldiering, once the honorable life of a brave man, has become largely a matter of armed thugs killing (or starving) civilians and trying to leave no witnesses to the actual violence. In a war zone, the opposite sides take turns, and the soldiers (government, guerillas, child recruits) are often safer than the non-combatants.
THERE HAS NEVER BEEN A WAR BETWEEN TWO GENUINE DEMOCRACIES. When a democracy and a non-democracy go to war, it has become the norm for the non-democratic side deliberately to place their own non-combatants, especially children, in harm's way so as to generate misguided sympathy.
People with agendas (especially the Left: J. Pub. Health. Pol. 19: 289, 1998) deluge us with claims that the United States is an extraordinarily violent society. (Our homicide rate is now 4.7 / 100000 people, 14827 homicides in 2013, along with non-fatal injuries from violence down by about half from the 1990's but still higher than the other developed nations -- update JAMA 314: 478, 2015 -- from age 1 to age 44, homicide is the most common cause of death among non-Hispanic blacks.) This ignores the fact that the violence is concentrated in underclass communities. These communities, for whatever reason, are lawless and ridden with substance abuse, and the "code of the streets" requires posturing ("keeping respect") that ultimately invites re-injury (Am. J. Pub. Health 95: 816, 2005). Monitoring serial admissions of "penetrating trauma recidivists" shows "it only gets worse", and that the manner (shooting, stabbing) usually stays the same until death occurs (J. Trauma 61: 16, 2006). Where there is not a culture of lawlessness, dependency, individual non-achievement, and despair, and where illegal drugs are not being dealt, people in the US are as safe as anywhere in the world (and safer than most places). Among "indigenous peoples" and in the slums of the poor nations, violence and murder are far more prevalent. Despite the "noble savages" claims of the Left, the evidence of archeology is every bit as horrorific (for example, Sci. Am. 289(2): 33, 2003).
In the late 1800's, the Belgians under megalomaniac
King Leopold II looted
the Congo, killing around 10 million people and enslaving, torturing and mutilating
many more. This prompted massive
outrage at the time in the US and Britain but has now been mostly
forgotten.
The genocide in Armenia (about 6 million dead) in the early 1900's
rarely gets mentioned. (In 1939, Hitler, preparing to "kill without pity or
mercy all men, women, and children of Polish race or language", said, "Who still
talks today about the Armenians?")
We almost never hear about
the slaughter of millions of civilians, especially in China,
by the Japanese military as the empire was expanding.
And they almost certainly did
experiment with germ warfare, including
plague
Whatever your politics, and whatever your specialty, you'll see the contents of this lecture during your practice. People who abuse alcohol, do drugs, choose a violent lifestyle, and/or do tobacco consume a grossly disproportionate amount of health care. You'll be very impressed when you go on rotations. When insurance-company talk of "health care cost control" turns to excluding sports injuries (as it sometimes does "because you assumed the risk"), I think of the incredible irony and stupidity.
NON-VIOLENT DEMONSTRATION: The participants will do whatever they can to get attention and ideally provoke a VIOLENT response from the people that they want the public to see, fairly or not, as "the bad guys." You've seen plenty of this from extremists and demagogues at both ends of the political spectrum. Often, it works. DEATH INVESTIGATION AND THE PRIMARY CARE PHYSICIAN
The first problem in any examination of death is find out whose body it was. Remember that identification of remains by distraught relatives is notoriously unreliable. The police will almost always do fingerprinting and/or dental identification. For skeletonized remains, the forensic anthropologist (a Ph.D. specialty allied to pathology) and the DNA lab (get the DNA from tooth pulp) can be extremely helpful. * Death is a great disguiser. -- Shakespeare. * Heads-up to country doctors called for a consult by the police -- it is quite common to find a partly-decomposed bear's paw in the woods. On x-ray, the bones look quite human except that the bear has several sesamoid bones that we do not.
Next, you may be asked to estimate the time of death. This is not an exact science.
* Post-mortem rectal temperature time of death nomogram: For. Sci. Int. 54: 51, 1992; the actual ranges vary hugely; post-mortem hypoxanthine For. Sci. Int. 51: 139, 1991; vitreous potassium For. Sci. Int. 46: 277, 1990 & AMFJP 18: 158, 1997; CSF chemistry J. For. Sci. 38: 603, 1993. All about post-mortem chemistry: Am. J. For. Med. Path. 14: 91, 1993. * Ed's time-of-death program gets thanks from police and prosecutors around the world. * A man convicted (very likely wrongly) of a godawful rape-murder based on unreliable estimates of how fast you digest dinner: AJFMP 12: 344, 1994. Scientific pathologists hate charlatans as much as scientific clinicians hate health-care quacks. For bodies found in the great outdoors, maggots are the medical examiner's little friends (more than you want to know about maggots: J. For. Sci. 38: 702, 1993).
{07024} maggots
In forensic pathology, histologic study of the tissues plays a very limited role. * Forensic nursing is an up-and-coming field. Nurses focused on forensics can pick up procedural errors in the hospital, and can excel at describing wounds at the time of presentation (which can be very helpful at trial). If the law does not require a medical examiner's inquest, or if you are the medical examiner, keeping the following in mind will help you avoid the usual pitfalls. The CAUSE OF DEATH is your best opinion, as a physician, with or without an autopsy. You list this on the death certificate. CAUSE OF DEATH: Thromboembolus in right main pulmonary artery (circa 1 minute) SECONDARY TO: Thrombophlebitis of leg vein (circa 5 days) SECONDARY TO: Adenocarcinoma of the pancreas (circa 6 months) NOTE: You may call the most important (to the lawyers) item on your list the "proximate" cause of death, i.e., what set the fatal chain of events in motion. "Cancer of the breast" is okay; "coronary artery atherosclerosis" probably isn't (why not?) NOTE: Please don't write "cardiopulmonary arrest" as the cause of death. We already knew that.... The MECHANISM OF DEATH is your story. "The Trousseau pulmonary embolus strained the right ventricle and a rhythm disturbance developed." Once again, this is your best opinion. The MANNER OF DEATH is for the lawyers. You might list your opinion on your death certificate, too. There may be future disagreement. In the above instance... MANNER OF DEATH: Natural Here are your choices:
SUICIDE: At the very least, the person did something that resulted in his or her death, and this was more or less what the person intended.
ACCIDENT: These deaths resulted from some kind of unplanned, unintended injury. They include most "therapeutic misadventures" (i.e., mishaps at the doctor's or dentist's). Notoriously, if sporotrichosis from a rose-thorn prick were to lead to death, it would be an accidental death. Among the grayest areas are "accidents" in the workplace due to employer negligence; many prosecutors now consider these to be homicides (Am. J. Pub. Health 90: 535, 2000). Animal attacks are accidents (fatal dog attacks are very rare Am. J. For. Med. Path. 32: 50, 2011). NATURAL: Death due entirely to disease or birth defect. (NOTE: "Unnatural death" means homicide, suicide, or accident.) Some medical examiners find the "naturals" most interesting... much like in a big university hospital, the clinical history enables the pathologist to guess the cause correctly before autopsy 65% of the time (J. Clin. Path. 61: 124, 2008). I'll accept "death from old age" if the person is over 90 and there's no signs of violence -- the cardiac ventricles are supposed to be more subject to rhythm problems. UNDETERMINED: You're an honest doctor and you know you can't really tell. This is a great category for normal-looking, 300-year-old skeletons found in the desert with negative toxicology, most cases of "sudden infant death syndrome" with no proper death-scene workup, substance abusers or organic-brain-syndrome people found at the bottom of the stairs ("did they fall or were they thrown?"), etc., etc. NOTE: If I wrongfully bite you, and you go to the hospital and are rightly treated with penicillin, and you die of anaphylaxis as a result of the penicillin injection, your death is probably a homicide -- my wrongful act set this unfortunate series of events in motion. NOTE: If a guy shoots himself, and spends six months in the hospital recovering, and dies of a pulmonary embolus from being at bed-rest for so long, it's still a suicide. NOTE: By common practice, if a guy has bad emphysema and blows out his lung trying to inflate his kid's balloon, it's "natural", not "accidental". NOTE: The good medical examiner always asks "Why today rather than yesterday?" especially when the only finding is serious-but-stable atherosclerotic coronary disease. NOTE: "Therapeutic misadventures" do not include the deaths that result from expected risks of today's powerful therapies. If someone dies of pseudomonas sepsis while undergoing a bone marrow transplant for leukemia, death is "natural", i.e., an not-unanticipated consequence of the illness and its treatment. NOTE: Physician-assisted suicide will be part (though hopefully still an infrequent part, thanks to more humane terminal care in general) of mainstream medicine when you're in practice. These deaths (along with today's discreet acts of euthanasia) will be registered as natural deaths. NOTE: If you find me dead in front of the TV, with a half-eaten greaseburger dripping over my fat paunch, stinking of tobacco, with a medicine cabinet full of statins and anti-hypertensives that you can tell from the dates on the bottles that I didn't take, and I have known 3-vessel coronary disease and have been complaining of angina, and you don't know something's amiss or see anything curious on examining my body or the scene, go ahead and sign me out as "natural; cause of death is atherosclerotic coronary artery disease". Yeah, a few tricky homicides probably get missed. NOTE: Although there is no need to point out the irony, deaths from oat cell carcinoma, heroin-shooter's endocarditis, cocaine heart, and Laennec's cirrhosis are "natural deaths". In particular, your lecturer would like to see a sixth category, "Illegal-drug abuse-related", because separating accidents, homicides, and suicides here is close to impossible.
{07135} morbid obesity, another contributor to "natural" death
* MODE OF DEATH is an unpopular word for what was apparent without a physician's full workup ("shock", "coma", "pulmonary edema", "sudden cardiac arrest", "pneumonia"). MORE ABOUT DEAD BODIES Timing...
3 hours... Lividity is usually obvious. 5 hours... Rigor is usually obvious. 10 hours... The body feels cold. 12-18 hours... Rigor is usually maximum. 24 hours... Rigor is usually starting to lyse; this can be later if it's hot out 2 days... Green discoloration (sulfurated hemoglobin) on the flanks 2-3 days... Green discoloration on the abdomen 3-4 days... Marbling of the skin begins (red discoloration of surface veins) 5-6 days... Epidermis separates from dermis 2 weeks... Bloated, lots of gas in tissues 3 weeks... Gas causes bursting of the organs, eyes bulge, tissues are soft 4 weeks... Semi-liquid, slime After a near-plateau of variable duration (as above, heat generated by anaerobic metabolism approximately matches heat loss), the body cools at one degree celsius per hour in the first 12 hours, then 1/2 degree celsius for however long it takes to get to room temperature. Circumstances (clothing, obesity, ambient temperature, mystery factors) alter this rate of cooling tremendously. Things happen very differently in bodies deposited in the water. There are frequent surprises. A newborn with near-zero internal body flora, and some other folks, may not putrefy. * Jack Kevorkian's original claim to fame was his attempts to use the optic fundi to determine time of death in very early cases: J. For. Sci. 6: 261, 1961; Am. J. Path. 32: 1253, 1956. You are already familiar with RIGOR MORTIS, one-time stiffening of the body after death. In addition to the conventional teaching that this is due to depletion of ATP with subsequent binding of actin to myosin, I suspect this is due at least in part to the influx of calcium through injured membranes. You also know LIVOR MORTIS (I say LYE-vorr; others say "LEE-vorr"; "lividity", settling of the blood; this becomes fixed/patterned after a while, and can tell you if the body has been moved.)
* Leave the arcana of decomposition ("adipocere grave wax burns like candle wax and accounts for the fragrant smell sometimes reported when certain old burials are re-opened") and the identification of decomposed bodies to us. Check the "electrolytes" handout for more on determining electrolyte status at the moment of death from analyzing the vitreous humor. Approach to the dismembered body: AJFMP 12(4): 291, 1991. "Cadaveric spasm" is instantaneous rigor, seen when death occurs with considerable muscular exertion (gripping something, as a branch in someone falling down a mountain) and/or major motor seizure and/or emotion (battlefield, torture).
{07558} livor mortis
THE MEDICAL EXAMINER'S OFFICE
The MEDICAL EXAMINER is a physician who autopsies, or has a pathologist autopsy, certain dead bodies. It is a government-appointed position.
Plenty of medical examiners are general pathologists. And in rural communities, physicians who are not pathologists can do this work, getting consultation as needed. By contrast, the CORONER is a government official who makes official rulings about the natures of particular deaths.
Elsewhere, the coroner may simply be a college student whose real job is completing routine paperwork, rubber-stamping the medical examiner's conclusions. And in others, it may be a funeral director, or way out in the country, whoever owns a truck and is willing to transport dead bodies. Laws involving coroners can be interesting, and in some jurisdictions, it's also the coroner's job to arrest the sheriff should he/she misbehave. Coroner systems have been gradually giving way to medical examiner systems over the past few decades, (JAMA 279: 870, 1998). Call me old-fashioned, but for a rural county, the familiarity of a police coroner may perhaps work better. If you, the licensed physician, are caring for someone and he or she dies of his or her disease, you fill out the death certificate and you needn't even notify the Medical Examiner's office. Certain deaths must be referred to the medical examiner / coroner. These include: If there is a bullet in the body, even from long ago and unrelated to the death, the medical examiner (or perhaps a surgeon) should remove it for ballistics examination. In a typical community, around 15% of deaths will fall under the medical examiner's jurisdiction, and of these, maybe 35-45% will get autopsied.
Where it's an obvious, non-questionable suicide, the medical examiner will at least attempt to obtain the bullet if there is one. I used to do more extensive autopsies when I could, in the hopes of finding some hidden physical disease (i.e., cancer of the pancreas, brain tumor) and if a woman, determine whether she was pregnant. It's only an hour or two extra work for me, and would make a lot of difference for the family. For deaths in fires, the medical examiner will at least examine the airways. Soot there says "alive at the time of the fire". No soot says "dead at the time of the fire" or "flash fire". If a driver dies after losing control of the car or bicycle, or a swimmer is observed to go under, I always did a complete autopsy in search of natural disease. If a body is discovered in the water, usually there will be a complete autopsy. The pathologist may take blood from both sides of the heart and check electrolytes. Of course, even without an autopsy, we'll usually take urine (by suprapubic puncture) and blood (femoral vein puncture is best) and check for drugs and alcohol. Where time of death is an issue, or there's a suspicion of diabetes or drugs, vitreous humor will be sampled. Hair samples (roots and all, please) are helpful for the drug history and more. Vaginal swabs and smears will be obtained on all possible homicides of women; oral and anal swabs from everyone.
Terminology: Whether the person is killed with a firearm or some other weapon, the pathologist examining the wounds will be asked, "Could this weapon have caused this injury?" The pathologist will examine CLASS CHARACTERISTICS ("Rope used in strangling will produce a bruise-abrasion like this one") and INDIVIDUALIZING CHARACTERISTICS ("This rope's twists and thickness exactly match the impression left on the victim's neck.") ANATOMIC PATHOLOGY OF CHILD ABUSE:
* The great forensic pathologist Ambrose Tardieu wrote an extensive account of physical findings in child abuse in 1860. It was ignored. The story of how we came to recognize the existence of "the battered child syndrome", and the decades of denial that such things could actually happen, is chronicled in Clin. Lab. Med. 3: 321, 1983. ("Isn't it strange how fragile some kids' bones were in life, but not after death?" "When you question the family, be sure not to say anything that might make them feel guilty." "This syndrome of 'osseous discontinuity' can be mistaken for trauma.") There is much appropriate discussion of "the battered child syndrome" with evidence of repeated past injury. But the majority of infanticides are the result of sudden anger by a frustrated parent ("I thought at least my BABY would love and comfort me"), and you will not find old trauma. Thanks to increased recognition by physicians, and increased awareness perhaps including parents themselves, deaths from child abuse have clearly decreased since the mid-1970's in the developed world (UK Arch. Dis. Child. 97: 193, 2012). In the "shaken baby syndrome" (review NEJM 338: 1822, 1998), an acute subdural hematoma follows avulsion of the subdural bridging veins. Look also for retinal bleeds and cerebral edema. You may or may not see a bruise (if the head has been struck; or the striking of the head caused the bleed.) One would think it'd be unnecessary, but it's not -- the worldwide "Don't Shake the Baby" media campaign of the early 1990's: Br. Med. J. 310: 344, 1995. Retinal hemorrhages are common enough just from getting born or even c-sectioned, but are almost always gone by 4 weeks (Ophthalmology 108: 36, 2001). Worth knowing: Of course, two fractures of different ages in a kid is probably child abuse. And any history that obviously doesn't fit the physical findings is pretty much diagnostic. There is no such thing as "temporary brittle bone disease". Babies simply don't get accidental fractures until they start walking by themselves. It's now clear that household / playground accidents can and do cause serious / fatal head injury -- very rarely (Dr. Plunkett, AJFMP 2001). This article provoked a firestorm of criticism from the ideologically-minded, but no scientific rebuttal so far, and it seems open-and-shut. Don't miss a torn frenulum, in life or at autopsy.
* Occasionally, psychotherapy helps violent people live better lives, but it's an uphill battle. Review of psychiatry and the treatment of violent patients: Arch. Gen. Psych. 49: 493, 1992. Chilling reading: The neurology of violence (Arch. Neurol. 49: 595, 1992). It is simplistic to attribute all violence either to biologic or sociologic factors. Major trauma cases (from Sherwin B. Newland, How We Die): 35%... automobile riders
Thalidomide caused the shortening of the limbs ("phocomelia") of unborn children.
Cancer chemotherapy in general is rough on the bone marrow, causing neutropenia and thrombocytopenia. You'll learn about specific agents in "Pharm". For now: Bleomycin, in high doses predictably cause pulmonary fibrosis. Cyclophosphamide causes a vicious urinary bladder inflammation. Adriamycin causes a cardiomyopathy. Vincristine produces a dysautonomia and painful, disabling peripheral neuropathy. Reserpine, a great anti-hypertensive drug, causes depression, and even suicide. Methyldopa and propranolol are also depressing. Phenytoin and cyclosporine produce hyperplasia of the fibrous tissue of the gingiva. Phenytoin and coumarin are notable teratogens. The mono-amine oxidase inhibitors can render a person highly susceptible to tyramine in strong cheese and wine, resulting in hypertensive crisis, brain hemorrhage, and so forth. The side-effects of glucocorticoids range from immunosuppression to osteoporosis to Cushingoid body habitus. What's more, going off glucocorticoids quickly is a good way to die of addisonian crisis (the adrenal cortex atrophies while exogenous corticosteroids are being taken). Several good anti-malarial drugs are oxidizers and will cause hemolysis, especially in patients with G6PD deficiency. Aspirin is rough on the gastric mucosa, renders all circulating platelets largely and permanently ineffective (until replaced in 7 days or so, of course), and (in overdose settings) produces a famous sequence of respiratory alkalosis followed by metabolic acidosis. The benzodiazepines are amnesic agents. (PLEASE don't prescribe these "to help people study.") So is scopolamine (and perhaps atropine). Caffeine produces a mild physical dependency, and withdrawal is accompanied by headache, drowsiness and lots of REM-rebound (sweet dreams....); see below. Penicillin at very high doses (i.e., meningitis) causes a non-immunologic hemolysis of red cells. If bromsulphthalein dye or adriamycin infiltrate out of the vein, you'll need a skin graft. Amphotericin B regularly causes acute tubular necrosis, which is so bad it tends to calcify. Cyclosporine, for renal and other transplants, is also a renal glomerular and tubular poison. Man problems often result from drugs (ask): Methyldopa, the classic anti-hypertensive, and opiates (prescribed, street) prevent erections. Clomipramine and the other selective serotonin-reuptake inhibitors make ejaculation much more difficult (dudes, this has its uses....) Thioridazine causes retrograde ejaculation, which can scare the guy. Anabolic steroids are fun but will (at least) accelerate your hair loss (more about gym steroids later). Spanish fly (cantharidin) is supposed to be an aphrodisiac for both you and her, but it's not safe (Forens. Sci. Int. 56: 37, 1992, or ask the Marquis de Sade, who was put away after poisoning some CSW's with it). Woman problems: Estrogens have a host of side-effects, the most alarming being the increased risk of atypical hyperplasias and (generally low-grade) carcinomas of the endometrium. Deep-vein thrombosis is an unpredictable but serious complication.
The alterations in lipid metabolism and fat distribution of the highly-effective anti-HIV drugs are now famous. In the past, "clever" murderers used digitalis / oleander extract, succinylcholine, sodium fluoride, or insulin to commit "the perfect crime". Today's savvy medical examiner can detect all this foul play. Here's this pathologist's personal list of "the most infamous" UNPREDICTABLE drug side-effects (i.e., nobody knows who will get them, the dose doesn't matter, and it's likely that the chaos of the immune system plays a role). "Are you allergic to any medications?" Penicillin is a great antibiotic and a great IgE sensitizer. Anaphylaxis following injected penicillin in a noteworthy complication. Quinidine, a good anti-dysrhythmic, causes sudden cardiac death in maybe 1% of people who start taking it. Clozapine (the epoch-making anti-schizophrenic drug) and phenylbutazone are noteworthy causes of agranulocytosis. Remember this risk for any drug you prescribe! Gold (for arthritis) and penicillamine (for Wilson's, scleroderma, etc.) are notable causes of glomerular protein leakage, often with devastating long-term effects. Nitrofurantoin, cyclophosphamide, bleomycin, busulfan, azathioprine, and amiodarone are lung poisons, producing ARDS or chronic interstitial pneumonitis, often at low doses. Methotrexate is prone to do the same; if you see non-caseating granulomas, suspect the methotrexate.
Amiodarone, griseofulvin, and isoniazid (ask the pharmacologists about "fast acetylators") are liver poisons. (Lots of other drugs can do the same.) The histopathology can mimic alcoholism. (Amiodarone is a horrid lysosome poison.) The non-steroidal anti-inflammatory agents are the most common cause of outpatient renal failure nowadays. The old sulfonamide drugs crystallized in the glomerular filtrate and cut up the tubules, while the classic NSAID-prototype phenacetin caused frank necrosis of the renal papillae. Halothane is a classic cause of massive hepatic necrosis in unlucky individuals. Overdosing on acetaminophen will do the same thing (big doses overload the safe metabolic pathway via glutathione, and a bizarre, toxic free-radical metabolite then forms by a second pathway -- update Clin. Tox. 50: 27, 2012). Hydralazine, procainamide and isoniazid often produce lupus (anti-histone disease, etc.) The first two are the worst. Methysergide occasionally causes retroperitoneal fibrosis, with obstruction of the ureters. Certain anti-malarial agents will blind occasional patients by causing a retinopathy. Abacavir, a very important anti-HIV medication, causes a frightening hypersensitivity syndrome; having a particular HLA allele seems to be required to get this, and antiretroviral therapy is now planned around this. Pretty much anything can give you a rash. Types range from IgE, type-I immune injury-mediated urticaria, to type IV mediated phenomena that follow presentation of the drug by Langerhans cells in the epidermis, to the serious vasculitis syndromes, to the dread toxic epidermal necrolysis. In the future, we'll know more biomarkers (i.e., genetic alleles) that correlate with different drug allergies (there are about ten known as of 2008: NEJM 358: 637, 2008.) {53779} phenytoin-induced birth defect, trust me
If all this alarms you, remember that Dr. Hippocrates had no specific drug prescription for any specific disease. Dr. Still and Dr. Osler didn't have a whole lot more. The three of them, unlike many of their contemporaries, realized the situation and had the integrity to say as much. Today's physician must weigh the benefits and risks of any prescription. NOTE: "The Physician's Desk Reference" lists side effects of drugs for the judge and jury, ranging from the probable to the improbable. Pretty much everything can supposedly cause "headache", "dizziness", etc., etc. THE ILLEGAL DRUGS
There's no room here for a major treatise on recreational drug abuse, but when you start seeing patients, you'll be impressed with the problems they cause. Uncle Sam (1994) reported that usage peaked in 1975, with 23 million users (i.e., people who'd taken a recreational drug in the previous month). Now that the public is more savvy (maybe), and people can lose their jobs if they flunk random drug tests (definitely), the count is down to maybe 11 million, but this is the hard-core. Your lecturer has been observing the drug scene since the sixties. IN MY HONEST, CONSIDERED OPINION, THE RECREATIONAL USE OF TODAY'S ILLEGAL DRUGS HAS NOTHING TO RECOMMEND IT.
Some of the essential pathophysiology remains mysterious. We don't even know why pulmonary edema is usual in opiate overdoses, or why people who do street drugs tend to have a hepatic triaditis and enlarged portal lymph nodes. Talc or whatever crystalline substance was present in the injected mixture often finds its way to the portal macrophages, which may also be pigmented.
* The most interesting work in this area, an examination of gene expression profiles in the nucleus accumbens, tends to discredit the recently-popular idea that the various addictive drugs work through a common pathway ("the addicted brain..."). See Neuropsychopharmacology 31: 2304, 2006. * The amygdalas (brain areas that have to do with self-control) in the experienced cocaine-user afflicted with craving seem much smaller than those of normal folks (Neuron 44: 729, 2004). Cause (weak-willed in the first place / stupid enough to try cocaine) or effect (damage from cocaine) or both? We are eagerly awaiting an answer.
Likewise, the medicolegal evaluation of the deaths of drug-users is fraught with pitfalls.
Tolerance, i.e., decreasing drug effect as the dose is held constant, makes it difficult to say whether the amount that the person took could / could not have been lethal. Illegal drugs and their metabolites are easily measured in blood and tissue after death, but post-mortem drug levels must not be over-interpreted. Especially, drugs redistribute after death in ways that so far have baffled the best forensic scientists (J. For. Sci. 44: 10, 1999). It's common for a drug, especially if it's lipophilic and there's a fair postmortem level, to be even 10x more concentrated in heart's blood than in femoral vein blood (Am. J. Clin. Path. 133: 447, 2010) as the drug dissociates from the molecules to which it's bound and enters the blood -- and if you see preposterously high levels of any drug after a long postmortem interval, consider this may be involved. Obviously as body proteins denature and temperature and pH change, affinities for the molecules change and drugs diffuse. Most forensic pathologists will simply tell you, "This lab result means the person did this drug." The specificities of your screening tests may be insufficient to detect particular drugs. For example, today's "opiate screen" is likely to miss fentanyl.
And of course, the drugs that were at the scene at the time of overdose are likely to be gone by the time that the police arrive. Terms to know:
BODY STUFFER: Someone who conceals the drug in a packet in the body before being arrested. Both types can show up in the emergency room very, very sick (J. Tox. Clin. Tox. 42: 987, 2004; Ann. Emerg. Med. 55: 190, 2010.)
Today, this euphoriant-anesthetic substance needs no introduction. Taken by needle, through the nasal mucosa, or smoked in heat-resistant form as "crack" (from the cracking sound made by the crystals), it's has long been major evil presence. There's a mild physiologic withdrawal syndrome. More seriously, once the drug is sampled, the psychologic craving is intense. Even experimenting a little with cocaine, even "to help you study", is extremely dangerous. Apparently cocaine use destroys your capacity to be happy without the drug. The cocaine addict will do anything to get more of the drug. In the 1980's, the introduction of a cheap, smokable form ("crack", from the sound of the blocks breaking as they burn in the pipe) caused a striking increase in use. According to Sci. Am. 290: 82, Feb. 2004, the use of crack dropped precipitously in the early 1990's. The author's explanation was that community leaders recognized that the danger to their communities' health was too great to accept as "politics and profits as usual", and "extra-judicial street justice" removed the crack dealers. Today's social scientists attribute the tremendous increase in crime between the late 1980's and the mid-1990's largely to the rise and fall of crack. Cocaine kills people in at least five different ways:
Cocaine and the heart: NEJM 345: 351, 2001; Am. J. Card. 100: 1040, 2007. It is adrenergically mediated and potentiated by both ethanol and tobacco. Cocaine depletes dopamine receptors on the coronary arteries, and renders them super-sensitive to alpha-adrenergic stimuli. This is most likely the cause of the vasospasm (Am. J. Card. 86: 1054, 2000) and symptoms and signs of cardiac ischemia. The cocaine-induced fibrohyaline thickening of the intramyocardial arteries was demonstrated early in this century.
Less well-known is smoked cocaine's ability to produce damage to the pulmonary microvasculature (Chest 121: 1231, 2002). Even if the patient does not have hemoptysis, this is one cause of a lung's being full of hemosiderin-laden macrophages. Check the blood for cocaine in any young person with unexplained hemoptysis.
Remember that even though the brain rapidly develops tolerance to the euphoriant effects of the drug, the sodium channels of the heart never develop tolerance to the effects of cocaine. This triggers rhythm disturbances and death. * People with one of the monoamine oxidase A alleles get impressive atrophy of the orbitofrontal cortex if they do a lot of cocaine (Arch. Gen. Psych. 68: 283, 2011). Pathologists look for these findings, which are typical of heavy cocaine users and to a lesser extent other stimulant users: (1) Replacement of single cardiac myocytes by fibrous tissue (probably why we get the diastolic dysfunction of the left ventricle; this is distinctive for "chronic catecholamine cardiomyopathy" of which cocaine heart is the chief example); (2) Medial hypertrophy, hyalinization, and/or fibrosis of the small coronary resistance arteries. (For a review with photos see South Med. J. 98: 794, 2005). Tachyarrhythmias probably result from the underlying anatomic changes in the heart, since (unlike myocardial infarction), they won't happen during the first experimenting. Brain hemorrhages happen even if the vessels in the head are "normal": Neurology 46: 1741, 1996; brain vessel constriction can also produce stroke: JAMA 279: 376, 1998. "Crack lung" produces a spectacular anthracosis. * You may be told that cocaine produces a vasculitis, especially in the brain (Neurology 40: 1092, 1990). I don't know whether this is true; most cocaine users get no vasculitis from the drug. So far as I've been able to find out, there's no distinctive lesion; it may be just a rare Stevens-Johnson drug-allergy vasculitis. Future medical examiners:
Cocaine is metabolized into benzoylecgonine (serum half life 6 hours, urine half-life 12 hours) and ecgonine methyl ester (serum half-life 4 hours); both degrade into ecgonine which is stable indefinitely. If there is also alcohol on board, about 10% of the cocaine will be turned into cocaethylene, a psychoactive compound with a half-life of 3 hours. Watch for post-mortem studies on brain receptors in cocaine addicts, to demonstrate and understand tolerance.
The famous perforation of the nasal septum is simply an ischemic infarct from vasoconstriction. Cocaine can also kill unborn children by abruption of the placenta or direct toxicity to the fetus (For. Sci. Int. 47: 181, 1990; still clearly true Am. J. Ob. Gyn. 204: 340, 2011), or make babies small and/or premature. Today's "crack babies" need no description (ask a pediatrician, or see Pediatrics 97: 851, 1996; these babies are significantly smaller Pediatrics 101: 229, 1998; Although the most dire predictions have not held up and non-crack-exposed underclass kids also have special problems (Pediatrics 98: 938, 1996; J. Ped. 132: 291, 1998), the "crack babies" do seem to have been damaged permanently by the drug (Pediatrics 120: e1017, 2007). * One future hope is a vaccine, i.e., a cocaine analogue that is immunogenic, producing antibodies that bind cocaine and prevent its having an effect. Hope it works. See Nature 378: 727, 1995; Proc. Nat. Acad. Sci. 98: 1988, 2001. Vaccines are also "under development" for nicotine, methamphetamine, phencyclidine, etc., etc., but after a decade there's been nothing really promising (Curr. Psych. Rep. 9: 381, 2007). EXCITED DELIRIUM is a curious phenomenon in which a person (most often on cocaine or amphetamines, though the blood levels need not be high and it's seen sometimes without drugs on board) requires physical restraint, then stops struggling and shows labored / agonal breathing and immediately goes into cardiopulmonary arrest. The syndrome is defined to be each of these in succession: (1) hyperthermia, (2) delirium, (3) respiratory arrest; (4) death. Nobody really knows the mechanism (Am. J. Emerg. Med. 19: 187, 2001). The phenomenon is so familiar to forensic pathologists and to the police that I have no serious doubt that it's real. The autopsy molecular signature is now reported to be elevated HSPA1B and much-diminished dopamine transporter (For. Sci. Int. 190: e13, 2009). Of course, excited delirium generates a lot of bogus "police brutality" lawsuits. Update on excited delirium deaths in custody, viewed with 20/20 hindsight back to 1939: AMFJP 30: 1, 2009. Of course, some of these people die WITHOUT being taken by police, in the way described above (J. Anal. Tox. 33: 557, 2009). Your lecturer suspects that excited delirium, rather than "police brutality", is an important mechanism of death when someone who the police hog-tie dies suddenly (Am. J. For. Med. Path. 31: 107, 2010), though it's possible that a fat person hogtied with a police officer on his back might have his guts pushed upward into his chest cavity, restricting breathing.
DOWNERS (barbiturates, others) Overdoses can be fatal, especially if you've had a drink. (NOTE: Your lecturer doesn't believe that it's common for people to "forgetfully" take the rest of the bottle of sleepers while groggy from taking just one.) For big-time abusers, there's a physical tolerance and withdrawal syndrome (excitement, seizures) that can kill you. Remember skin blisters in people in "barb" coma; nobody knows why they happen. Gamma-hydroxybutyrate (gamma hydroxyburytic acid), gamma-butyrolactone, and 1,4-butanediol (the latter is an industrial solvent, yuck) are popular yuppie downers. Gamma-hydroxybutyrate mimics GABA, the inhibitory neurotransmitter, and crosses the blood-brain barrier easily. Again, there's a physical dependence and the risk of acute toxic death (NEJM 344: 87, 2001).
Even old-fashioned sedatives such as chloral hydrate still kill people.
The benzodiazepines ("Valium", etc.) are amnesic drugs. You won't learn well while you're taking the stuff "for test anxiety" or anything else. Today's "more sophisticated" exam-takers are choosing propranolol, a drug with effects on the heart that are not always salutary. Put that stuff away, too. * Even the anesthetic propofol is now being used by people seeking a relaxant; it turns out tobe addictive (Clin. Tox. 48: 165, 2010). UPPERS The amphetamines ("speed"; most-used right now is methamphetamine; update Mayo Clin. Proc. 81: 77, 2006) are rough on the heart (sudden death is famous; also "meth cardiomyopathy" Am. J. Med. 120: 165, 2007; disturbingly common Am. J. Card. 102: 1216, 2008), brain, and kidneys, and may incline their users to do foolish, hurtful things. However, sudden deaths from these substances are uncommon, and tend to mimic cocaine's anatomic pathology.
Compared with the other drugs of abuse (except ethanol), "meth" is much more likely to lead to death or serious injury by making its users violent and reckless. Of course, we are in the midst of a "meth" epidemic, and folks in the emergency room in San Diego are more likely to be on "meth" than even marijuana (J. Trauma 63: 531, 2007). Probably no one was surprised to learn that cocaine and methamphetamine users get horny and do reckless sexual things (Am. J. Psych. 164: 157, 2007). The famously-bad tooth decay and fractured teeth seen in the methamphetamine user is caused by a combination of xerostomia, the noxious smoke ("crystal meth" / "ice"), bruxism, and a craving for sugar (Am. J. Health-Syst. Pharm 63: 2078, 2006; Gen. Dent. 54: 125, 2006). It's hard to show in the lab, but your lecturer believes that vasoconstriction from the drug probably infarcts the mouth tissues -- your lecturer thinks this is the main cause of "meth mouth". Like "crack babies", "meth babies" born to women who did methamphetamine are much smaller than their counterparts. We await follow-up (Pediatrics 118: 1149, 2006; confirmed Ob. Gyn. 116: 330, 2010; J. Ped. 157: 337, 2010). Phencyclidine's pathology is being worked out. It's been a challenge as specific lesions haven't been found, and it's hard to know who's been using. The NIH finally starts looking at folks' "true addiction history" by hair samples, but this isn't feasable for your limited-budget medical examiner (Addiction Biology 13: 105, 2008). Mephedrone is an amphetamine available as tablets; it famously causes bruxism (tooth grinding); it's resurfaced and is now being made illegal. (For. Sci. Int. 206: e93, 2011).
3,4-methylenedioxymethamphetamine ("Ecstasy" / MDMA) is a familiar yuppie drug whose problems are now being studied intensively.
A curious effect is hyponatremia, as the drug seemes to cause both inappropriate secretion of ADH and inappropriate water drinking. This is now a robust finding (Am. J. Med. Sci. 326, 89, 2003; Ann. Emerg. Med. 49: 164, 2007), and can be lethal. Use of MDMA is common, deaths from MDMA are rare, and they usually resemble other amphetamine-type deaths (Legal Med. 9 185, 2007).
* In 2011, synthetic chemicals were marketed in stores as "bath salts", supposedly to be put in your bathwater rather than be consumed as the amphetamine-like drugs that street people knew they were. They killed a few people, caused some appalling senseless violent outbreaks, resulted in quite a few speed-like emergency-room visits, and are now being made illegal (Clin. Tox. 49: 499, 2011; MMWR 60: 624, 2011; NEJM 365: 967, 2011). Compare New Zealand's "party pills" (piperazines): Clin. Tox. 49: 131, 2011. * Not really uppers: KETAMINE has caused surprisingly few deaths in recreational users, who are likely to be medical types. See Int. J. Leg. Med. 116: 113, 2002. * Not really uppers: LSD and mescaline are seldom encountered today (which is good); there is no known anatomic pathology (Clin. Tox. 48: 350, 2010.) {07615} tattoo on public-spirited person
It's commonplace for an "accidental" overdose to have been preceded by a critical life-event, and many of these "unfortunate tragic accidents" are probably suicides (Forens. Sci. Int. 62: 129, 1993) while others may have had a recent brush with the law and the dealer gives the buyer an uncut dose of drug to produce the death of a possible business liability. * Confusingly, there is an illness seen only in people who snort cooked heroin, and that much be due to some other poison generated in this way. It looks clinically and anatomically like prion disease, but some patients recover; it's called "heroin spongiform encephalopathy" and is recognizable now on MRI scans: For. Sci. Int. 113: 435, 2000. Social scientists tell us that heroin was responsible for the upsurge of crime, especially robberies, from the mid-1960's to the mid-1970's. Methadone maintenance as a readily-available treatment proved a great help (thanks very much for that one, Mr. Nixon). Methadone / suboxone maintenance keeps drug addiction, which is a relapsing problem, under partial control with great savings to society. There are about 100,000 people on methadone maintenance in the US, and only about 500 deaths per year from overdosing. Most deaths result from increasing the initial dose too rapidly. You'll review the various molecules in "Pharm". It's worth remembering that heroin is diacetylmorhine and is metabolized to morphine. Don't try too hard to interpret a post-mortem morphine level, either to decide whether "it's enough to kill the person", or how much of the drug was taken. Tolerance varies tremendously, and attempts to second-guess tolerance by high-tech assays of brain receptors have been non-helpful: For. Sci. Int. 113: 423, 2000. During life, 98% of a dose of opiate is in the tissues; as the body decomposes, much of it will return to the bloodstream. Review J. For. Sci. 46: 1138, 2001. Redistribution is less of a problem than for other drugs: J. For. Sci. 45: 843, 2000.
* Don't forget to look for pupa cases from the maggots that fed on the body. Morphine can be analyzed from here: For. Sci. Int. 120: 127, 2001. "Big Robbins's" statement that a third of heroin addicts had diluted their drug with water from the
toilet comes as no surprise to this physician. Heroin may be cut with Baby's talcum powder (stays in
the lungs forever), quinine (rough on the heart), or whatever else is handy (who knows?) Heroin
addicts seldom use sterile technique, and abscesses and endocarditis (notably on the tricuspid valve,
notably staphylococcal It's worth remembering that tolerance to opiates is lost VERY fast. One common scenario is a fatal overdose after a 2-3 day stay in jail; the addict simply took the customary dose and died as a result (for example, the death of Sid Vicious). Savvy medical examiners are now estimating these people's tolerance history using hair samples. Ultra-rapid detoxification, which ends the addiction during a few hours of artifical sleep and naloxone treatment, has been available since the 1990's and the military (i.e., reality-based) now uses it for burn victims (J. Trauma 71(1S): S-114, 2011).
Ask a forensic pathologist to show you needle marks ("tracks"). These are scars, often pigmented (carbon, hemosiderin), overlying veins and often arranged in a line (savvy dopesters start distal). One reason addicts get tattoos is to make it harder to see their injection sites. "Skin poppers" are often covered with old craters.
{08170} heroin tracks
People who inject "Ritalin", "Talwin" or methadone from powdered tablets are also certain to get interesting stuff in their lungs. Talcum powder and pill-fillers both produce little granulomas, which can eventually cause fatal cor pulmonale.
* Buprenorphine implants for the treatment of opiate dependence: JAMA 304: 1576, 2010. The management of patients with chronic pain is only now receiving the recognition it deserves from the medical profession, and is still restricted by laws that don't make sense (a fact that is finally getting media attention). Heroin may perhaps have some use in the management of chronic pain, but the discussion is totally dominated by ideological concerns. Today, however, most users chose heroin not for a physical analgesic but as a powerful anesthetic against deplorable living conditions. It works (and this would lead me to ask why so many people feel they need it -- perhaps the cause is having to live around other substance-abusers, criminals, and mean people), but the problems only begin with impotence, constipation, and infections. * For the not-pretty picture of both TB {07062} talc in heroin-abuser's lung
Baudelaire, Toulouse-Lautrec, Van Gogh, and Rimbaud were devotees of the drug, which raises the question (for me anyway) whether their devotion to the drug was the cause of, or the result of, their particular outlooks on life. The movie "Moulin Rouge" (2001) celebrates the hallucinations generated by absinthe. A Jayhawk argues that VanGogh's psychosis was at least exacerbated by his absinthe: JAMA 260: 3042, 1988; more by this author on absinthe: Sci. Am. 260(6): 112, June 1989. The special ingredient that produced the weird intoxication is supposedly thujone. If you believed everything you read about this, you'd be reading uncritically. Despite its molecular resemblance to the active ingredient of marijuana, it doesn't work on the cannabinoid receptors. More credible is work showing that it acts on the GABA type A receptors (Proc. Nat. Acad. Sci. 97: 3826 & 4417, 2000). This suggests excitotoxicity as the cause of the permanent brain damage. * The sad story of a man who drank wormwood obtained via the internet: NEJM 337: 827, 1997.
The familiar weed, which archeologists tell us goes back at least to the 6th millennium BC, binds to particular receptors in the brain, as do most other drugs. Today, there are as many marijuana smokers as tobacco smokers in the USA (JAMA 307: 173, 2012). The active agent is delta-9-tetrahydrocannabinol. Ask a neuropharmacologist about the "cannabinoid receptors", and the endogenous cannabinoids, notably N-arachidonoylethanolamine (charmingly named "anandamide", ananda being Sanskrit for "bliss.")
* Formerly the hemp plant was cultivated widely in the US for
rope and canvas (same word as "cannabis").
People seeking rational explanations for our curious marijuana
laws have suspected the political influence of
the cotton industry ("King Cotton"; canvas clothes are less
comfortable but more durable) and of course the big liquor companies.
Or (and this seems right to me) this is just another example
of "the law of alien poisons", i.e., that every dominant culture abhors
the mind-altering substances preferred by its minority groups, and cannabis
was primarily used by Hispanics who called it "Mary Jane" (Substance Use and Misuse 37: 853, 2002: from Nova Southeastern COM).
Something on this history of the international ban on marijuana, with a reminder
that it was largely driven by a disinformation campaign by a single US politician:
Lancet 313: 344, 2004.
The "medical marijuana" laws are inadequate to
provide the obvious benefits the drug offers (NEJM 362: 1453, 2010);
but even the Bush administration (October 2009) reversed itself and stopped
sending the Feds after people using the drug in accordance with their
states' medical marijuana laws.
There is a mild withdrawal syndrome seen only in heavy users (i.e., four or more joints per day) that lasts less than a month, with the ex-stoner losing weight, sleeping fitfully, and being crabbier ("increased aggression" shows only on lab tests that seem to measure irritability): Am. J. Psych. 161: 1967, 2007. In one long-term study, stoners who weren't already crazy were somewhat more likely to go crazy ("exhibit psychotic symptoms") than non-stoners -- cause and effect, or effect and cause? You decide (BMJ 342: d738, 2011). Right or wrong, the government crusade against marijuana has long been a part of "politics as usual". Marijuana smoking was a "political" act during the 1960's, when the government's several "credibility gaps" were obvious and many people were given absurdly long prison terms simply for possessing a joint or two. It seemed to make its known users unmotivated, and your lecturer suspects this means it causes subtle brain damage that may or may not be reversible. If the latter is really true, it has resisted scientific demonstration. * Ironically, at the same time that
marijuana was the drug of choice for the 1960's, mostly anti-Vietnam-war
"counterculture",
it was also the drug preferred by front-line troops during the war,
who preferred it to alcohol since they wanted to be able to fight effectively in case of surprise attack.
* Government and government-promoted (D.A.R.E.) material for young people
about
the supposed risks of marijuana includes obvious, preposterous untruths.
For example:
* Of course, this undermines the credibility of warnings about dangers
of heroin, cocaine, methamphetamine, and the other genuinely-life-threatening drugs.
In the US, politics-as-usual includes the maintenance of an illegal drug culture
among the poor and the stupid, with marijuana as the gateway drug.
Draw your own conclusion.
Your lecturer makes yearly medline searches that always reveal exactly nothing plausible about serious health consequences of marijuana smoking (beyond an ultra-rare, Buerger-like "cannabis arteritis" (Br. J. Derm. 152: 166, 2005; J. Am. Acad. Derm. 58(5S1): S65, 2008; the Germans reviewed the data and decided there was no such thing Vasa 39: 43, 2010). NOR CAN THIS WRITER IMAGINE HOW THE NEUROLOGIC "AMOTIVATIONAL" SYNDROME (if it is real) COULD BE CLEARLY DISTINGUISHED FROM THE APATHY AND ENNUI OF SPOILED MODERN-DAY U.S. KIDS. This includes the effort in JAMA 287: 1123, 2002, in which Aussies who smoke weed daily for decades have progressive impairment of memory and attention (thanks for trying). Even the Canadians, not known for liberalism, found that the supposed stupidity (i.e., lowered IQ) of stoners is measurable only in those smoking five or more joints weekly, and that looking at past users, "we conclude that marijuana does not have a long-term negative impact on global intelligence" (CMAJ 166: 887, 2002). A mega-study involving imaging of the brain of young teens found smaller brains in those exposed to alcohol, to cocaine, and to tobacco -- but there was no demonstrable effect from marijuana (Pediatrics 121: 741, 2008). In 1999, Bethesda funded a huge study on medical marijuana; it is reviewed in Arch. Gen. Psych. 57: 547, 2000 -- after a lot of hearings and calls for more research, the one solid recommendation was a metered inhaler rather than just letting the patient smoke the weed as a joint. (No, this doesn't make sense to me, either). Studies showcasing the common-sense idea that marijuana helps with chronic painful illnesses continue to be published in major journals (Neuro. 68: 515, 2007 -- the patients are now allowed to smoke the stuff; CMAJ 184: 1143, 2012 finds smoking cannabis much superior than placebo for difficult-to-manage pain and spasticity in multiple sclerosis.) The 2002 claim that cannabis smoking causes 30,000 deaths in Great Britain seems built on faulty assumptions -- you decide: Br. Med. J. 327: 165, 2003. Contrast this with a study from JAMA 299: 525, 2008 indicating more periodontal disease in stoners independent of tobacco use -- without considering that perhaps stoners do not brush-floss their teeth so often as non-stoners or perhaps even eat more candy. How frankly nonsensical the world marijuana laws are: Lancet 363: 344, 2004 (again, not a bastion of liberalism). Mayo's rightly points out that the ongoing hoopla is driven by politics without huge, rigorous studies on either side (Mayo Clin. Proc. 87: 172, 2012) -- but how could science NOT take a back seat to something that has been an important part of our culture for the past sixty years? You should not smoke cannabis and then drive a car (reminder BMJ 344: e536, 2012). This was "prove-able" only after blood assays for marijuana smoking became available. See Lancet, April 24, 1976, page 884. A group of Canadian academicians conducted a phone survey asking (1) "Do you drive your car when you are high on marijuana?" and (2) "How many fender-benders have you had?" They discovered that people who drive stoned average twice as many wrecks (no surprise: Traffic Injury Prevention 11: 115, 2010). * In 1997, a team in Italy noticed that cannabis and heroin both activated mesolimbic dopamine transmission by a common receptor mechanism. The subsequent claim that this suggested marijuana was addictive met with guffaws; it seems to me that it simply reflects the fact that both drugs make people happy while they're high (Science 276: 1967, 1997; this would not be worth mentioning except that it got published, somehow, in this distinguished journal and you may hear about it.) Nobody seems to have trouble stopping marijuana smoking. Of course, marijuana use results in very few domestic-violence calls. Contrast alcohol. It's also very widely reported to be easily the best way to overcome the dreadful subjective side effects of cancer chemotherapy. This is intensely politicized (your chemotherapy patients will try it themselves, and probably not tell you). Even Canada, not known for radical social politics, legalized medical marijuana in 2001. Your lecturer hasn't seen anyone physically sick or dead from marijuana, and believes that claims of grave health threats, birth defects, and so forth are simply disinformation. The few people who are actually getting sick smoked stuff that's been adulterated (for example, by levamisole: Arth. Rheum. 63: 3998, 2011 -- we can't prevent this as long as it remains illegal). Nor has your lecturer heard of dreadful harm from countries where marijuana is available legally at convenience stores. Even the new edition of "Big Robbins" trimmed its warnings against marijuana down to concern about smoke damaging the lungs and being stoned making your thinking fuzzy. Smoking several joints daily is somewhat rough long-term on the lungs but occasional marijuana use seems not to cause lung troubles (JAMA 307: 173, 2012) and using a water-bong is probably safer (JAMA 307: 1796, 2012 -- but where are we going with this?) JAMA 287: 1172, 2002 confirms what everybody knows -- even 17 hours after getting zonked on marijuana, your head's not quite clear. The JAMA editors, not known for being left-wing, also pointed out that most current work does NOT really support the idea that marijuana causes long-term brain damage, and that it's also impossible to tell in any case whether people who smoke a lot of dope are stupider to begin with. (You think?) Science takes a back seat to politics, and truth be told, almost nobody's doing meaningful scientific work with marijuana use itself today. This is a shame, since (for good or ill) the drug is a well-established part of U.S. culture, and (because it is illegal) might be purchased from the same kind of folks as the much more dangerous drugs (i.e., kids learn how to buy from drug dealers). Plus, the brain systems on which it works are evidently quite important (Nat. Med. 9: 1227, 2003). A review of adverse health effects of non-medical cannabis use (Lancet 374: 1383, 2009) emphasized the lack of any real science. The one strong recommendation is to not drive a car when stoned. * Synthetic cannabinoids ("Spice herbal incense") that actually do work on the cannabinoid receptors (Eur. J. Pharm. 659: 139, 2011) are now being made illegal (For. Sci. Int. 208: 47, 2011).
* Why do you THINK they call it "dope"? -- Ed
THE INHALANTS ("glue sniffing", etc.) Some people have fun inhaling solvents (acetone, ethyl acetate), gasoline, isobutane (cigaret lighter fluid Int. J. Leg. Med. 120: 168, 2006); isobutyl-, amyl- and butyl-nitrites ("pig pokers", etc.), nitrous oxide ("Whippets", from aerosolized whipped cream cans; a yuppie favorite), toluene (airplane glue), and fluorocarbon (J. For. Sci. 38: 477, 1993) propellants. Solvents probably act (like general anesthetics) by solubilizing the lipid in nervous tissue and acting on the same proteins as anesthetics do. Use of some of these drugs can be bad for the heart (sensitizes to rhythm disturbances), kidney, and brain. Intoxicated people can die of aspiration or asphyxia. Nitrous oxide users are prone to develop a peripheral neuropathy and megaloblastic anemia. "Huffing" is now popular, with computer-cleaner sprays and air-conditioning fluid. "A cool way to die." See Am. J. For. Med. Path. 33: 64, 2012. * My favorite article from 2007 was the account of the autopsy of a sniffer of toluene from paint. Granules of aerosolized paint in the lungs were magnificently demonstrated on electron microscopy (For. Sci. Int. 171: 118, 2007). 
There's no time or reason to dwell on the arcane, political-legal subject of testing for drugs of abuse. Worth knowing: Heroin is metabolized to morphine, and cocaine to benzoylecgonine and ecgonine methyl ester. You measure these. RULE: If there's to be a legal impact of your findings, you must confirm all positives using a test based on a different chemical principle. * It is possible to test meconium to see whether Mom has used drugs during pregnancy. Early work (J. Ped. 122: 152, 1993) suggested this might become routine, but understandably it's primariy a research tool, though it has finally come into widespread use (Pediatrics 118: 1149, 2006; Arch. Dis. Child F&N 91: F291, 2006; Clin. Chim. Acta 366: 101, 2006; For. Sci. Int. 153: 59, 2005).
One fact that needs to be understood by a society considering de-criminalization of marijuana is the fact that it remains detectable in the user's urine longer than more dangerous drugs. People who want to party on Friday night but will lose thier jobs if they are found "drug-positive" on a random urine check on Monday know this, and are more likely to use meth or cocaine instead.
Interdicters, moralists, "educators", certain (not all) "drug counsellors" (tough-talk, warm peer
support, and monitoring costs mega-bucks for rich professionals or medicaid-recipients caught doing
drugs; I'm told "alcohol rehab" now costs $30,000 even though AA's / NA's,
still the best, is still free), and (of course) drug dealers all have vested
interests in keeping this "war" (and addiction itself) going rather than making timely physician-directed treatment available.
An issue I have with one-size-fits-all "drug rehab" programs is that they
do not address the other life-situations, i.e., an abuser who can't read or has
no useful skills won't get help with this, and there's little emphasis on
teaching other living skills that might actually make the person independent
and not need either drugs or the revolving rehab door as a crutch.
If Newt and Bill ("a new advertising campaign against drugs for 1998")
had really wanted to end the problem, it would be possible for any
strung-out addict to present himself/herself for humane treatment
(for example, an ultrarapid opioid detoxification using naloxone and
artificial sleep: JAMA 279: 229, 1998). Is this available?
Ads for it are just starting to appear. The strung-out addict is going to rob somebody instead.
It is easy to recognize politically-motivated, futile escalation
(remember Vietnam?), war-profiteering, or how the current policy of
ensuring that drugs generate
crime (and crime-profits) serves politics-at-its-worst for both right-wingers
and left-wingers. Bill Clinton
actually talked about "harm reduction" (JAMA 273: 1143, 1995) rather than a "war"
we can win, and the British (not known for being soft-hearted)
already consider "damage control" and not "fighting drugs" is
the only rational option (Br. Med. J. 315: 329, 1997).
Stay tuned (Sci. Am. 269(1): 24, 1993; CIBA Found. Symp. 166: 224, 1992.)
Jocelyn Elders, M.D., was pilloried for suggesting decriminalization; a
few years later, Newt Gingrich said the
same thing and no right-wingers got upset.
Your lecturer, while no expert on social policy, believes that addiction is bad. Yet I would prefer
accessible treatment of addiction (how much does humane detoxification and ongoing monitoring,
without other frills, have to cost, anyway?), some ongoing public education (it doesn't have to cost
much, and by now everybody knows, anyway...), and other reasonable incentives (as with ethanol --
remember Prohibition? alcohol abuse probably went down after it was repealed; and this doctor will
give you a urine specimen anytime you like, thank you) instead of the continued emphasis on
attempting to enforce laws as a means of containing what is a very serious problem.
Other physicians are now coming around to your lecturer's position
as well (Acad. Med. 70: 355, 1995). Maybe the
"Smokers' Rights" proponents might make the logical step to drug decriminalization. Amsterdam,
where drugs are legal and treatment is readily available, hasn't exactly become a horrible place to
be.... Even the British Medical Journal (312: 1655, 1996), not exactly a hotbed of radicals, is now
calling the "war on drugs" a defeat, and calling for decriminalization and even legalization.
The British, who speak more candidly about affairs in the US than our own medical press,
seem very happy with Mr. Obama's ideas, including (1) ending the ban on
federal funding for people who exchange needles; (2) no raids on people
growing medical marijuana legal under state law; (3) drug courts for
non-violent offenders. See Lancet 373: 1237, 2009.
The Obama administration maintained the interdiction policies while
focusing on reducing demand for drugs and treatment for drug misuse --
by 2012, Mr. Obama's treatment programs had reached 22 million drug misusers
(Lancet 379: 1184, 2012. Decriminalization of the hard drugs isn't
discussable in the USA yet, but Mexico and the Central America are
seriously considering it given the damage caused by by the drug-driven wars.
As always, you're welcome to disagree.
OTHER NOTABLE POISONS Hanging onto bitterness and resentment is like eating poison and expecting somebody else to die. THALLIUM poisoning requires a very high index of suspicion whether or not it has been fatal, unless the distinctive sign has appeared -- hair loss, * perhaps preceded by blackening of the hair roots.
ORGANIC MERCURY is acquired from environmental contamination, particularly in high-on-the-food-chain fishes. "Minimata disease" was a dread neurologic syndrome among Japanese who ate fish caught near a mercury dump site. Selective necrosis of the tips of the granular layers of the cerebellar folia is the signature lesion.
{07026} mercury poisoning
A widespread, subtle, chronic poison, primarily in industrial exposure (including those who must live near China's lead mines: Am. J. Pub. Health 101: 834, 2011) and Nigeria's new child gold miners (400 deaths so far, crime against humanity -- Lancet 379: 792, 2012), moonshine, and among children who eat the sweet lead paint chips in slum housing (or inhale paint dust from the windowsill -- still a major problem Am. J. Pub. Health 101-S1: S115, 2011). An episode in medical history that has been more or less overlooked was the epidemic of lead poisoning from the placement of lead pipes (hence the name, "plumber") to supply water to houses. The dangers were recognized in Europe as early as 1850, but the epidemic of disease in the US was still going strong as late as the 1930's (Science 315: 1669, 2007), thanks primarily to a massive disinformation by the Lead Industries Association (Am. J. Pub. Health 98: 1584, 2008). We are still paying the price. Many houses built before 1960, especially those built on the cheap, are full of lead paint. Remodelling can be unhealthy in these homes, even if nobody eats the paint. Beware also of the paint dust around where the windows open. "The environmentalist community" alternates between activism and indifference. In countries where there's still leaded gasoline, folks who get high by inhaling the stuff get sick from lead poisoning. Lead in the quack calcium supplements: JAMA 284: 1425, 2000. In quack Asian remedies: Clin. Ped. 50: 648, 2011. You can also get lead poisoning from a retained bullet / bullet fragments (Pediatrics 117: 227, 2006). Lead poisoning from smoking marijuana adulterated with lead pellets to increase the weight of the bag (NEJM 358: 1641, 2008). "Pencil lead" isn't lead, but graphite. The lead accumulates in bone, where it will remain for a long, long time. Supposedly, lead acts by scrambling disulfide groups. In any case, it affects many systems. In the blood, a hypochromic-microcytic (why?) anemia results from interference with porphyrin synthesis (delta-ALA dehydratase and ferroCHELAtase; old typo in "Big Robbins".) Future pathologists: Look for basophilic stippling, where chunks of ribosomes remain bound in the red cells. In the kidney, it produces a Fanconi syndrome. (Future pathologists: Look for acid-fast, hyaline intranuclear inclusions.) It also poisons the ability to the kidney tubule actively to secrete uric acid, producing the famous "saturnine gout". (* The old Roman character "Saturn" was, among other things, patron of lead.)
{07019} lead inclusions in nuclei of renal proximal tubular epithelium In dirty mouths, lead joins the mercaptans of bad breath to produce the famous "lead line" at the gums. (Future physical diagnosticians: you can see the "lead line" in bismuth and mercury poisoning, too.) Lead produces an encephalopathy. This can range from learning and behavioral problems of young kids, through horrible cerebral edema, seizures and death in older folks. Lead also produces a myelin-and-axons peripheral neuropathy. The chronic, colicky abdominal pain of lead poisoning is infamous. The mechanism probably has something to do with lead being taken up at the presynaptic terminals through calcium channels. In 1991, the CDC recommended screening all one-year-olds and two-year-olds for lead poisoning (Pediatrics 93: 201, 1994). In the poor neighborhoods, no reasonable person would question the value of this screening.
* An assertion that subclinical lead poisoning is a major risk factor for hypertension flopped: JAMA 275: 363, 1996. ARSENIC (Lancet 347: 1596, 1996) Then she began to groan, faintly at first. Her shoulders were shaken by a strong shuddering, and she was growing paler than the sheets in which her clenched fingers buried themselves. Her unequal pulse was now almost imperceptible. Arsenic, the popular crime-fiction poison and spirochete-killer, disrupts oxidative phosphorylation, ties up sulfides, and does other things. Arsenic trioxide is colorless, odorless, and tasteless, and has always been a favorite for homicidal poisonings.
* When he finished his internship, Michael Swango MD got his revenge on his attending staff using arsenic, but nobody died that time. Swango's long career as a serial killer was enabled mostly (it seems to me) by physicians' fear of being sued.
Acute poisoning -- when not fatal in very short order -- is most noxious to the gut, causing vomiting, bloody diarrhea, and severe pain in the abdomen. This progresses to death in hours or days. Chronic poisoning causes an encephalopathy, neuropathy, and abdominal pain. Look for (1) hyperkeratosis of the skin, particularly the palms and soles; these may turn into squamous cell carcinomas; (2) "Mee's lines", white smooth lines in the fingernails, where arsenic is bound to keratin (you can see these in renal failure after chemotherapy too -- contrast Beau's depressions, after any grave illness); (3) basophilic stippling of the red cells. (4) Look for blackening of the hair roots too. Arsenic is normally present in ground water. After deeper wells were drilled in Bangladesh as an intended public service, water rich in arsenic was struck, and much concern resulted -- see Lancet 360: 1757, 2002; J. Tox. 39: 683, 2001; Lancet 376: 213 & 252, 2010. * A famous double-death suspected to be arsenic poisoning is proven to be such: BMJ 333: 1299, 2007. * "Paris Green", the famous arsenic-based pigment used in wallpaper in the 1800's, released arsene gas when mold grew on it during the damp season. ("Damp weather is unhealthy!"); * "Holistic medicine!" Dangerous levels of mercury and arsenic in "Chinese herbal medicine" NEJM 333: 803, 1995. 
{07121} Mee's lines
* COPPER toxicity, from old-fashioned containers, was almost certainly the cause of an epidemic of childhood cirrhosis in kids who inherited an (autosomal recessive) susceptibility gene (Lancet 347: 877, 1996); I predict this will be found to be the cause of "Indian childhood cirrhosis" as well. PARAQUAT This famous weed-killer will, if swallowed, causes ARDS ("acute pulmonary fibrosis") and death over days or weeks. This is among the dumbest possible choices as a means of suicide. When the Carter administration sprayed it on Mexican marijuana fields, U.S. marijuana smokers became wildly and selectively indignant over the possible threat to their health. (* "We smoke pot! We like it a lot! So stop spraying it with paraquat!") Paraquat murders: AJFMP 18: 33, 1997. * Unripe tropical akee fruit contains dicarboxylic acids (remember the pathophysiology of Reye's?) which cause a fatal encephalopathy (Lancet 353: 536, 1999). * CHLORINATED HYDROCARBON INSECTICIDES (DDT, dieldrin, others) I think that I shall never see /
The risk-benefit profiles of these chemicals, especially DDT, is the subject
of disinformation campaigns by both the Right and the Left.
The chemical was virtually banned worldwide in the mid-1970's.
Banning DDT altogether became a huge cause in the 1990's
for the environmentalist movement,
culminating in the Johannesburg agreement. The Clinton administration
took up the cause.
Thanks to spraying with DDT in the 1950's,
the United States and Europe no longer have
a malaria
The supposed health risks of DDT -- even living next to the dumpsite
and having the stuff in your water supply (Env. Health. Perspect. 108:
1113, 2000) resist demonstration. The osteoporosis claim flops
(Arch. Env. Health 55: 386, 2000). The study that DDT residues
triple your breast cancer risk comes from an organization of which I've never heard
(Cancer Causes & Control 11: 177, 2000); the NIH study was negative
(Cancer Causes & Control 10: 1, 1999), and so was the Johns
Hopkins study (Cancer Ep. 8: 525, 1999). The NIH looks at lymphoma
and does not find a connection: Occ. Env. Med. 55: 522, 1998.
"No convincing evidence that organochlorines cause a large excess
number of cancers" --NIH Annual Rev. Pub. Health. 18: 211, 1997.
The NEJM wrote a scathing account of "paparazzi science" underlying
anti-DDT activism (337: 1303, 1997).
Nature Medicine stated bluntly that the ban was driven by
rich "green" activists for their own political gain, "balancing risks
on the backs of the poor" (Nat. Med. 6: 729, 2000).
Most recently, several individuals (all from identify-environmental-poisons
organizations I'd never heard of) presented a claim that prolonged industrial
exposure to DDT causes brain damage. I can't see this in their own
small-sample statistics, in which
differences between
exposed and non-exposed people are small and on some tests the exposed
people did better than the controls, and demonstrably sick people were eliminated
from the control group but not the sample group
(Br. Med. J. 357:
1014, 2001). Frankly, the corruption is obvious.
A bigger study will surely be forthcoming.
DDT sometimes acts as an estrogen. You can make a fertilized boy
fish egg grow up into a girl fish if you inject a gigantic
amount of DDT into it (Env. Health Perspect 108: 219, 2000).
But if DDT demasculinizes human or other warm-blooded males, I couldn't
find anybody writing about it.
Even the World Wildlife Fund's spokesperson (Br. Med. J. 321:
1404, 2000), who claims children need to be protected both from malaria
and from DDT, cites no credible recent work to show a real danger from
the latter; his major
citation is Am. J. Pub. Health 77: 1294, 1987 which found a very
weak correlation between DDT levels and shorter duration of lactation
which has never found any further support.
If you
check his reference on "endocrine disruption" (J. Clin. End. Metab. 85:
2954, 2000), that author merely mentions that this is an allegation made by some people.
South Africa's DDT workers basically have no troubles with sperm counts or
anything else sexual (Env. Res. 96: 1, 2004).
An huge attempt to link DDT exposure to low birth weight did not achieve
statistical significance (Am. J. Epid. 162:
717, 2005).
In 2005, a retrospective study on the mental development of babies exposed in utero that failed to control
for other variables (which was probably impossible anyway) gave mixed results
(Pediatrics 118: 233, 2006); since DDT is present in breast milk and actually
seemed to benefit this cohort, perhaps DDT is not the cause. Everything else is even softer.
However... the pesticide leaves residues in the environment that stay
around for a long time. This can't be wholesome, though an
adverse impact on humans
(if any) isn't clear so far.
Contrary to right-wing claims, university wildlife
experts do still believe that the ban on DDT brought the
bald eagle back (Env. Health Rep. 103(S4): 51, 1995; also
Science 218: 1232, 1982), and
the stuff seems to interact specifically with the steroid
receptors on the glands that make
eggshell.
Even the World Wildlife activist admits that malaria continues on the rise,
killing at least a million people yearly (low guesstimate) and making 300 million people
sick. And insecticides are key to its control.
But DDT is pretty much out of use anyway in favor of
better chemicals, except in the poorest countries.
Most of the world uses better, somewhat more expensive chemicals.
I suspect this is why the Clinton era saw a chance to look good by calling for a ban on the stuff --
the non-evidence-based environmentalists could make their political capital without being
justly
accused (that time) of indifference to one of the world's worst genuine
health problems.
Update: Johannesburg is forgotten. By 2006, even Greenpeace and the World Wildlife
Fund decided they were in favor of using DDT where it's really needed
(India, sub-Saharan Africa). DDT is most useful in spraying homes
and on netting. This obviously saves lives and
seems to generate much less resistance than widespread
spraying (Am. J. Trop. Med. Hug. 71(S2): 214, 2004).
Only a few extremists still campagin against this.
ORGANOPHOSPHATE INSECTICIDES (malathion, parathion) Like the chlorinated hydrocarbons, intoxication may be acute or the result of accumulation in body fat. These drugs are basically acetylcholinesterase inhibitors, i.e., first you'll twitch, then go limp (why?). You'll find a full discussion in the section of a "Pharmacology" textbook that also deals with myasthenia gravis. Some of them are so toxic that a few drops on unprotected skin will kill. (A famous outbreak a few years ago was caused by a bottle spilled during trucking onto blue jeans later sold in a department store.) You'll recognize these patients by their having a mysterious illness with drooling and pinpoint pupils. The decreased serum cholinesterase levels seen in life remain reliable during the hours following death, if the cause of a "sudden and unexplained death" is not obvious. Worldwide, the most common method of suicide is self-poisoning with pesticides (commonest of course in the poor nations; estimate is around 300,000/year; Lancet 369: 169, 2007; Clin. Tox. 50: 202, 2012). * Future pathologists: A point-of-care four-minute test for red cell acetylcholinesterase to check for organophosphate poisoning is now available (Ann. Emerg. Med. 58: 559, 2011). GULF WAR SYNDROME, i.e., neuropathies and minimal-brain-dysfunction problems, may have resulted from exposure to chemical weapons, pyridostigmine, flea collars, etc., etc., etc. This will never get sorted out. See JAMA 277: 215, 223 & 231, 1997.
POLYCHLORINATED BIPHENYLS ("PCB's") If you believed everything you hear about the alleged dreadful effects of these pollutants, you'd be listening uncritically (to put it mildly). Those who work with them don't have any obvious pattern of illness. The disturbing thing, however, is that they almost completely resist degradation in the environment, and it's hard to tell who has how much on board and to control for variables. Stay tuned to find out what real damage (if any) they will do us. DIOXINS (nice review: Am. Fam. Phys. 47: 855, 1993; nothing on adverse effects is being published any more) These include "agent orange" (the Vietnam herbicide from "Operation Ranch Hand") and the stuff in the West Virginia Nitro and Italian Saveso industrial disasters, and were among the "Love Canal" pollutants. They also are produced in small amounts by most combustion, and they tend to accumulate in the food chain and thus in people (Am. J. Pub. Health 84: 439, 1994 for levels). "Agent orange" contained a trace of * 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), which is the semi-poisonous stuff and seems to be a cancer promoter like so many other chemicals. The manufacture of all dioxins is now banned in the U.S. for political reasons. * The story about "dioxin" or TCDD being the most poisonous substance known just isn't true. Guinea pigs are allergic to the stuff, which is most of the basis for this claim. TCDD is a "carcinogen" (probably just a promoter) and teratogen in some animal systems. In big doses, it can kill an animal soon after administration, but this hasn't been reported in humans. A few weeks after heavy exposure, a human's sebaceous gland basal cells undergo metaplasia into keratinocytes, pushing sebum out of the follicle in huge horny blobs ("chloracne"). This gets somewhat better in a few months or years. In 2004, Ukrainian politician Viktor Yushchenko was poisoned during his candidacy, with the intent of rendering him ugly. It worked, and he ended up gaining sympathy votes and getting elected president. Most of the Vietnam Vets who were actually exposed took part in a single fiasco ("Operation Ranch Hand"). These folks now turn out to have about 50% more basal cell skin carcinomas than other comparable folks, but no demonstrable increase in anything else so far. Nobody's been able to show an increase in birth defects among children of exposed service personnel from Vietnam (or Saveso or Nitro survivors), nor has convincing evidence of an epidemiologic link to human cancers been forthcoming. Studies finding nothing: NEJM 324: 260, 1991; Am. Rev. Resp. Dis. 144: 1302, 1991; JAMA 267: 2209, 1992; Arch. Int. Med. 150: 2845 & 2495, 1990; and those already cited in the Neoplasia chapter. More: Epidemiology 9: 161, 1998 (no increase in preterm babies, infant morality); Epidemiology 6: 4, 1995 (Air Force finds nothing to suggest negative reproductive outcomes); Epidemiology 7: 352, 1996 (no measurable effect on sperm counts, testosterone, etc.); One study does find a link between adult-onset diabetes, and exposure (history, blood dioxin assay; same Air Force lab as above): Epidemiology 8: 252, 1997. And it turns out that most Vietnam veterans don't even have any more TCDD on board than do civilian controls (Am. J. Pub. Health. 81: 344, 1991), though some do. The public continues to believe that Agent Orange is a major health hazard. In 1994, the widow of a chain-smoking Vietnam vet was awarded a large, precedent-setting pension because her husband's lung cancer was supposedly caused by agent orange. Serious interest in "Agent Orange" among real epidemiologists has dropped spectacularly since the mid-1990's. Some scientists who worked with the EPA on its "1994 dioxin report", which proclaimed that, yes indeed, dioxin was a big danger, denounced the whole thing as politically-motivated junk science (Science 266: 1629, 1994 -- still good reading). As one who honors the warriors (if not every war), I regret the exposure of our people to a carcinogen, and the campaign of fear and obvious misinformation. * Love canal: Chemicals from an old toxic waste site resurfaced. The locals were understandably and justifiably upset and angry. Fortunately, nobody has been able to show a statistically significant increase in any health problem (Science 226: 1217, 1984; Am. J. Forens. Med. Path. 3: 343, 1982; Science 212: 1404, 1981). One little-discussed after-effect of this sort of thing, and the legislation and litigation it has spawned, is that if you purchase a plot of land, YOU become liable for cleaning up any real or imagined toxic health hazard that some militant might claim to discover. As a result, certain locations cannot possibly be developed economically, and everybody loses. TOADSTOOLS (Pub. Health Rep. 126: 844, 2011) AMANITA PHALLOIDES, the "death angel" produces AMINITIN, which inhibits RNA polymerase. Death results from hepatic necrosis. Mostly an old-world mushroom, it's also present in the USA (Clin. Tox. 49: 128, 2011); the Americas have several species of galerina toadstools that also contain the poison. AMANITA MUSCARIA produces MUSCARIN(E), prototype of the parasympathomimetic drugs. ("SLUD" strikes again.) Expect to survive. TRICHOTHECENE: A potent mycotoxin that binds to the 60-S ribosomal subunit and prevents
peptidyl transferase from acting. This was the poison of the
* The homicidal poisoner: reviews AJFMP 17: 282, 1996,
AJFMP 16: 223, 1995; AJFMP 34: 38, 2013.
* The "milk sickness" that killed Abraham Lincoln's mother
and thousands of other early-USA pioneers resulted from
dairy cattle eating white snakeroot, which contains an alkaloid
poisonous to humans.
* Fun to know! Tea in China goes back at least to 2700 BC. "The English drink tea" because it was considered patriotic after they displaced the Dutch as chief imperialists in China. As the American Revolution was beginning, tea became a symbolic issue, and ever since, Americans have preferred coffee. Coffee itself was supposedly discovered by an Arab goatherd, who noted the goats became frisky after eating the berries. Its use became popular among Benedictine monks, who needed something to stay awake during marathon prayer sessions. Of course it was considered a drug menace when it became popular in Europe in the late 17th century; England's Charles II tried to ban it without success, and Bach's Coffee Cantata describes a 1730's father's effort to rescue his daughter from coffee-drinking, only to discover that the new beverage is in fact safe and delightful. Chocolate was a gift from the First Americans, while the kola nut came from Africa. In spite of what you've heard, caffeine simply does not produce measurable sustained hypertension (Am. J. Card. 73: 780, 1994; and once again Am. J. Clin. Nutr. 94: 1113, 2011). Nobody's been able to show any convincing risk for atherosclerosis, heart attack (Arch. Int. Med. 152: 1767, 1992), stroke, or sudden death. * There was a flap in the 1990's over caffeinated coffee drinking (two or more cups per day) and osteoporosis in women. However, the effect vanishes if the woman also drinks a glass of milk each day, and this finding makes me think that some other variable, not coffee drinking, is the cause. See JAMA 271: 280, 1994. Update, finding a risk in older women: Am. J. Clin. Nutr. 74: 694, 2001 (happens if they have the bad vitamin D receptor, which makes sense). * There's another longstanding concern over caffeine use and fetal loss. This might be real, but it isn't a huge effect See JAMA 270: 2940, 1993 and Am. J. Pub. Health. 82: 85, 1992 (makes the claim), JAMA 269: 593, 1993 (refutes the claim, and also denies that babies are more likely to be growth-retarded). NEJM 343: 1839, 2000 found a slight effect, but only if the woman is a non-smoker (study shouts "recall bias!"). In another NIH study, only extreme caffeine abuse (as evidenced by massively-high serum paraxanthine levels) was any risk for fetal loss (NEJM 341: 1639, 1999). Baby does experience the same enhanced wakefulness and diminished sleep that Mom does if she takes coffee: Am. J. Ob. Gyn. 168: 1105, 1993. Caffeine use isn't a risk factor for prematurity: Am. J. Pub. Health. 82: 87, 1992). In an update, the effects of caffeine as a cause of miscarriage are anything but impressive (Ob. Gyn. 98: 1059, 2001). The Dutch found that women drinking more than six "caffeine units" per day (seems like a lot) tended to have smaller babies -- real effect or confouding variables (Am. J. Clin. Nutr. 91: 1691, 2010). Of course, to cover yourself you'll still have to warn your patients to stop taking caffeine as soon as they find they are pregnant. * Caffeine is used to stimulate preemies to breathe and happily we now know it does NOT cause brain damage (! JAMA 307: 275, 2012). The alleged link with bladder cancer just doesn't hold up (Lancet 341: 1432, 1993). I'm very skeptical about the supposed link to pancreatic cancer, since it's inconstant and tobacco is likely to be a confounding factor. An attempt to show that maternal caffeine consumption during pregnancy causes attention deficit disorder in the child (you can't blame folks for wondering) failed (Am. J. Psych. 160: 1028, 2003). The alleged link with mouth and tongue cancer is anything but impressive (Cancer 70: 2227, 1992). The alleged link to rheumatoid arthritis as refuted (Arth. Rheum. 48: 3055, 2003). The pop claim that caffeine exacerbates fibrocystic change in the breast has consistently failed to hold up to controlled studies (J. Am. Diet. Assoc. 100: 1368, 2000). Caffeine use during pregnancy has been linked to SIDS but only if you fail to control for these women also being smokers, drinkers, and underclass (Arch. Dis. Child. 81: 107, 1999). More recently, the pop claim that it causes atrial flutter / fibrillation flopped (Am. J. Clin. Nutr. 81: 578, 2005). The medical community has finally documented what most adults already know: caffeine enhances the jitteriness of falling and low blood glucose (Ann. Int. Med. 119: 799, 1993). * Generalized anxiety disorder patients shouldn't take coffee (Arch. Gen. Psych. 49: 867, 1992), but it's okay for panic-disorder patients (ditto). We'll talk about the headache of caffeine withdrawal (probably the most common headache) under CNS (Mayo Clin. Proc. 68: 842, 1993). All about caffeine withdrawal, for those not acquainted with this: NEJM 327: 1109, 1992. Yeah, this means there's "a mild physical addiction", but despite occasional excitement about this fact from ideologues, no one has trouble breaking a coffee habit.
* Noah needed a drink when the flood waters receded, and made an "ass" of himself, becoming the "butt" of his son's joke (Genesis 9:20). And so sin "reared" up once again. See also Matthew 11:18-19 (drink or abstain, people will criticize you).
"Proof" (whiskey, other hard liquor) is double the percentage of ethanol in the bottle. Eighty proof whiskey is 40% alcohol. * We don't know how ethanol produces its buzz; there's only a little work and it involves GABA receptor channels (Proc. Nat. Acad. Sci. 92: 3633, 1995). Older ideas, which still might be right, focused on solubilization of ethanol in the brain lipid and the corresponding physical changes. The liver metabolizes alcohol first to acetaldehyde (via alcohol dehydrogenase), then to acetic acid, and ultimately to carbon dioxide and water. (* Microsomes and peroxidase-catalase systems also help handle some alcohol.) There is no question any more that heavy alcohol use by itself can and does permanently damage the brain. The problem's not so much that brain cells are destroyed (that's largely bunk) but that they are damaged ("loss of dendritic spines"). Check out Alc. & Alc. 25: 467, 1990; Exp. Neurol. 106: 156, 1989; still valid Brain Res. 1134: 148, 2007. Alcohol has traditionally been cited as causing about half of auto fatalities. Thankfully, today it's considered correct and even smart to choose one partygoer as designated driver. This participant remains cold-sober. (Try it. You'll probably enjoy it.) It takes about 5 beers or 5 shots of 80 proof liquor in rapid succession for the typical 70 kg man to reach the "legal" level of intoxication (100 mg/dL), but impairment of judgment and coordination occur at much lower levels. Watch for a lowering of acceptable driver's blood alcohol levels to 50 mg/dL or even lower. "The books" cite blood alcohol levels of 350-500 mg/dL as "fatal", but there's lots of variability. It's commonplace for a driver to be arrested with a blood alcohol of 300 md/dL or more. A chronic alcoholic may also die with a low blood alcohol "from cardiac rhythm disturbance brought about by alcoholism." Most people metabolize alcohol at a rate of 15 mg/dL/hr, using basically zero-order kinetics. That means you burn off about the equivalent of 1 beer or 1 shot of the hard stuff in 1 hour. Habitual drinkers handle the stuff much more rapidly, and there's much variability among people (for example J. For. Sci. 38: 104, 1993).
If the blood alcohol level is higher than the vitreous level, probably death occurred before equilibrium was achieved, i.e., the dead person had not been drunk for long.
In a putrefied body, the blood alcohol level can be as high as 150 mg/dL; a day or
so of decomposition can raise it up to 50&nbdp;mg/dL but usually not higher.
For the first day, there will be alcohol production only
if bacteria / candida Alcohol passes rapidly through the gastric mucosa, so if there's even 5 g/dL of alcohol in the stomach, the dead person had a drink within an hour prior to death. Alcohol in the stomach is prone to diffuse into the nearby heart and great vessels; moving the body may also cause some to be aspirated into the lungs with the same effect. Your best blood to sample for alcohol comes from the femoral vein. Take a sample from the vitreous also. The ratio of urine alcohol to blood alcohol can help you guess whether the person was actively drinking prior to death. If the ratio is under 1.2, the blood alcohol was probably rising at the time of death. If it is over 1.3, the person was probably drinking over a longer period of time.
* The long-term results are not salutary for either partner, but every adult knows that alcohol
is an extremely effective short-term anesthetic against nagging
and verbal abuse. This is a very
common step that leads to the chronic domestic violence syndrome. You might be able to teach
both parties a few new ways of coping, Doc.
* One major concern of a drinker and/or druggie considering sobriety is the loss of friendships. Don't
worry. Drinking "friends" will be replaced by higher-quality friends in the sobriety movement. This
is well-known by now, and makes me wonder whether people drink (do drugs, join stupid political
and ideological movements, etc.) because they are really seeking friendship. One thing your lecturer
likes about skydiving is that nobody's drunk or on drugs -- and a group of substance-free chums is
hard to find among today's grown-ups. Subclassification of alcoholism, simplified: Type I: Crybabies ("At least I'm not a criminal") Type II: Criminals ("At least I'm not a crybaby")
* You'll learn on rotations about naltrexone and other agents to reduce craving. Historical article: JAMA 281: 1318, 1999. Anyone overcoming alcohol dependence, regardless of kind or type, deserves our heartiest admiration and congratulations. For alcohol assays on the living or the dead, send us blood in a gray-top (sodium fluoride anti-bacterial, anti-enzyme) tube. Keep your sample frozen or in the refrigerator. Future pathologists: You'll use both (1) alcohol dehydrogenase methods and (2) gas chromatography for alcohol assays. The former detects methanol and isopropanol also; the second does too, but distinguishes them from ethanol. Remember that early decomposition can produce alcohol levels up to 50 mg/dL. "Alco-Screen" dipstick to measure the alcohol in spit: Ann. Emerg. Med. 18: 1001, 1989. Here's a partial listing of the bad health consequences of prolonged heavy drinking:
We're only now figuring out how alcohol affects the brain at the molecular level. Post-mortem alcohol levels are fraught with interpretive problems. Alcohol diffuses post-mortem from stomach to heart's blood. Bacteria from the gut reach the bloodstream by 6 hr, or faster if the gut is injured, and ferment glucose, especially if it's warm and/or there's a high blood glucose. This won't exceed 50 mg/dL the first day, and is usually much less, but can get to 200 or more if there are several days for decomposition. Be sure you also get a post-mortem vitreous sample (always possible) and a post-mortem urine sample (usually possible), and draw your blood from the femoral vein rather than the heart.
--W.C. Fields METHANOL ("wood alcohol", "blind, vomiting, and drunk") is metabolized to formaldehyde (yeah, you know that's gotta be bad for you) and thence to formic acid (which gives the famous high anion gap acidosis). The retina toxicity from formic acid is infamous ("like stepping into a snowstorm") and can be persistent. Part of the treatment involves saturating alcohol dehydrogenase with ethanol.
ISOPROPANOL ("rubbing alcohol", users are "rubby-dubs", etc.) is about twice as potent an intoxicant as ethanol, but really nasty to the gastric mucosa. Metabolized to acetone via alcohol dehydrogenase, and produces a modest anion gap acidosis.
ETHYLENE GLYCOL (anti-freeze) is metabolized to glycolaldehyde, glyoxylic acid, and oxalic acid. This stuff produces both a striking anion gap acidosis, and little crystals that carve up renal tubules, meninges, etc. Not a nice way to die.
* A locally-produced cough syrup, laced with ethylene glycol, killed around 100 Haitians (JAMA 279: 1175, 1998). {07016} ethylene glycol fatality; note crystals in the renal tubules
FIREARMS (Arch. Path. Lab. Med. 130: 1283, 2006)
* Currently, the "politically correct" stance for physicians seems to be to urge their patients to give up gun ownership. People even talk about such "firearm counseling" as a duty of the primary care physician (for example, South. Med. J. 103: 151, 2010, which points out the already-obvious fact that a gun in an unstable home is more likely to harm a family member than scare off an intruder). The push for mandating physicians to do anti-gun counselling sparked a media circus in 2011 and a Florida law.... But you already know this. Before you decide this is your duty, please read South. Med. J. 94: 88, 2001 about your possible liability issues should you use your position as a physician to pursue an anti-gun agenda. If you, as a clinician, understand gunshot wounds, your documenting them may be great help in eventually preventing a miscarriage of justice. It's a topic that's important but gets missed in undergraduate medical education (AJFMP 24: 273, 2003).
1. The flaming gas travels for a few inches and will produce a BURN. Carbon monoxide from the gas may impart a redness to the tissues surrounding an entry wound. 2. The soot travels for a few more inches (6-7 with most handguns nowadays) and will produce a SOOT MARK ("fouling"), which you can wipe off. Take your photo, wipe, and re-photograph. Of course, soot may be missed if the body is washed or hair shaved prior to full examination. Future pathologists: Look for soot and blood spatter on the hand that fired the suicidal bullet. If it's not there, this may be a "clever" homicide instead.
3. The unburned powder travels for up to a few feet (3 feet is usual for a handgun), and produces the POWER STIPPLING or POWDER TATTOO (not "powder burns", please; these are typically embedded in the skin so you cannot wipe them off). Ball powder gives bigger marks than the more common flake powder. {07249} powder tattoo around an entry wound 4. The bullet will enter (or graze) the body. If it enters, it will scratch the surrounding skin, producing the ABRASION RING.
TIGHT CUTANEOUS ENTRANCE WOUNDS: The muzzle is held against skin or clothing so tight that the gas, soot, and powder pass right through the broken skin. If the blast enters a confined space (i.e., a tight-contact gunshot wound against the calvarium or zygomatic arch), you'll see a star-shaped ("stellate") entry wound, as the skin is turned backwards and lacerated. There may be a muzzle imprint from recoil of the weapon. LOOSE CONTACT CUTANEOUS ENTRANCE WOUNDS: The muzzle is held at the skin, but not pressed hard against it. You'll see a small amount of soot at the edges, but there's no room for the powder to spread out for a dispersed tattoo. Again, there may be a muzzle imprint. Stellate bursting is less likely, but can occur. INTERMEDIATE CUTANEOUS ENTRANCE WOUNDS (6"-3' or so) If the bullet wound isn't a tight contact wound, and there's no soot, the shot probably came from several inches away. If there's powder stippling, you're probably within a range of three feet or less. The more dispersed the powder, the greater the distance. Test-fire the weapon and ammunition again. The soot and/or powder tattoo may tell you the direction of the shot.
Most entrance wounds are round, or a bit oval if the bullet entered at an angle. An irregular shape suggests that the bullet had lost its spin (i.e., passed through something else before entering the body) and "wobbled" on striking the body. EXIT WOUNDS may be produced by primary or secondary missiles. Exit wounds can have any shape -- round, stellate, slit, crescent, etc., etc. Note that you won't see an abrasion ring here. One pitfall is a "shored exit wound", an abrasion around the exit wound due to the victim was leaning up against a hard surface or the bullet hitting an unyielding piece of clothing, i.e., a leather belt, JFK's collar and necktie knot, etc.) If there's still any doubt about entry vs. exit wound, look at the clothing and check for residue. INTERNAL INJURIES As the bullet passes through the body, its energy is received by the tissues and dispersed in radial fashion. A temporary cavity is created with a diameter many times that of the bullet. Within 5-10 thousandths of a second, the cavity collapses, but the damage has been done. Organs that are not elastic (liver, spleen) are especially likely to be disrupted. The faster the bullet, the worse the damage. In injuries from rifles (except the lower-velocity .22 caliber type), most of the damage is due to the temporary cavity. A permanent cavity may remain behind. If the bullet exits the body, it will carry some of its energy with it, sparing the tissues. If the bullet yaws (i.e., tilts) as it enters the body, more energy will be dispersed over a shorter area. The configuration of the bullet, the length of the track, and the nature of the tissue struck all determine the seriousness of a bullet wound. Bullets may fracture bones. Wounds to flat bones (skull, sternum, rib) are usually beveled, with the direction of the cone pointing in the direction from which the bullet came (physics, with variations, J. For. Sci. 38: 339, 1993). Fractures of the skull often radiate from the bullet hole, and/or the supraorbital plates shatter like eggshells (the latter leads to "raccoon eyes").
As a matter of fact, if you spend time on the medical examiner's service, you'll be impressed how hard it is, generally, to kill a healthy young adult. Your lecturer once autopsied a gentleman who was stabbed through the heart, severing both descending coronary arteries and piercing the septum, and the descending aorta; the gentleman ran four city blocks before he fell down. Supposedly the brain can remain conscious for maybe 15 seconds after blood flow stops (ask Louis XVI). "Suicide by cop": J. For. Sci. 45: 384, 2000; Ann. Emerg. Med. 32: 665, 1998. Someone wanting to die does something to cause a police officer to shoot them. It is fairly common, and the reasons for the choice are obvious. SHOTGUN INJURIES (you can't just call these "gunshot wounds"; review Am. J. For. Med. Path. 28: 99, 2007) A close-range shotgun injury is the most destructive of civilian gunshot wounds. Why? (1) The weight of the pellets, and the energy in the gas, is very great. (2) The pellets almost never leave the body, so their entire energy is used damaging tissue. Close-range shotgun wounds to the head almost always cause it to burst. Close-range shotgun wound elsewhere recall cookie cutters. At greater distances, the shotgun pellets fan out. At 3-4 feet or so, the edges will be scalloped. At great distances, many will miss the target. This makes range the key to the severity of the shotgun wound. Shotgun pellets fan out on impacting the body, so you cannot tell the range from the x-ray. Look at high tightly-packed the entry wound is instead. At distances of two meters or less, the plastic / cardboard-cellulose wadding may end up in the wound. It's easiest to find on CT scan since it is radiolucent.
Multi-gunshot wound suicides (could have fooled somebody): AJFMP 10(4): 275, 1989. Suicide by gunshot while driving (the author correctly notes that more than a few auto "accidents" are actually suicides; AJFMP 10(4): 285, 1989). * THE KENNEDY ASSASSINATION: Lee Harvey Oswald, sharpshooter and left-wing kook, and/or companion(s), fired three shots from the Book Depository.
The first bullet missed, struck the pavement, and sent a bit of concrete flying, cutting a spectator's
face.
The second bullet passed into the back of President Kennedy's right shoulder, produced a stress
fracture of T1, came out the front of his neck just below the larynx (perforating his shirt collar and top of
the necktie, which shored the edge leading the inexperienced pathologist to mistake
this for the abrasion ring of an entry wound), then
went through the right side of Governor Connally's chest, and ended up in the governor's thigh. If
you say a single bullet isn't likely to do this kind of thing, you don't know what you're talking about.
The president's upper body lurched and his arms flexed in reaction to the spinal injury, creating the
impression that his head was being forced backwards by a shot from the front.
The bullet was rolling when it struck the governor, which is why the entry wound was large.
The third bullet struck the president in the back of the head, sending blood and 70% of the right
cerebral hemisphere splattering. The entry wound in the back of the head was small, and the exit
wound in the right parietal bone was six inches across. The head was first pushed forward, then the
seizure and jet effect of blood and brains forced the head back, again creating the false impression of
a shot from the front.
Nobody looked at the president's back at Parkland, and they didn't notice the head wound until
his heart had just about stopped completely. The guy who intubated him saw blood in the trachea,
so a Dr. Perry did a tracheostomy. In doing so, he obliterated the neck wound, which he also
unwisely speculated to be an entry wound.
The autopsy was performed at Bethesda amid much excitement.
It was a tough job, and it is clear
from the report that the pathologists were not really allowed to do
their job.
Partly because of
pressure from Bobby and Jackie, the pathologists did not shave the
scalp around the head wound (!), did not examine the spine or
describe the kidneys or adrenals
(!!) or the clothes (!!!) or the neck
organs (!!!!), and failed to note whether there was an
abrasion ring around the entry wound from the second bullet.
They claimed they could not establish the trajectory of the bullet that caused the back wound, and
later speculated that something fell out on the way to Parkland.
Bits of the parietal bone were later found on Dealey plaza, beveled out, confirming it was an exit
wound.
Back in the early Vietnam era (1963), the federal executive branch was secretive.
The Feds impounded the x-rays and autopsy photos, and
the pathologists had to rely on their own (faulty) memories for the positions of the head wounds.
Some important evidence got shredded early-on. Things are better now with this aspect of
government behavior, thanks mostly to the social changes of the later 1960's and early 1970's.
The conspiracy theorists focus on reporting rumors, claims by cranks, idle speculators, and even
obvious crazies, and failing to report other key facts. The single pathologist (Dr. Cyril Wecht) who
dissents from the Warren Commission's report was already a longtime conspiracy buff.
"Unexplained deaths of people connected with the assassination" mostly aren't unexplained. They
are the unnatural deaths of crooked or nutty people, or the natural deaths of other people. The
conspiracy buffs listed the people who died during the next few years and calculated the odds against
all these people dying around the same time. This is a classic misinformation-artist's fallacy: Flip a
coin 100 times, select only the times it came up "heads", then figure the odds against a coin coming
up heads each of 50-or-so times. Anyway, many of the "unexplained deaths" were of people friendly
to the Warren Commission and/or only peripherally involved. And after 30 years, no one has come
forward to confess, nobody has been caught murdering witnesses (which according to the some of
the conspiracy theorists has continued over the decades), and Oliver Stone produced his farrago of
lies ("JFK") without being molested.
People who know guns tell me that they don't believe that a lone assassin
could have gotten off three shots so quickly.
For more on the Kennedy assassination, see J. Am. Coll. Surg. 178: 517, 1994 (the governor's coat;
the exit bulge was too small to have been produced had the bullet not passed through the president
first); JAMA 267: 2791, 1992; JAMA 268: 1736, 1992; JAMA 269: 1540 & 1544, 1993.
The neurosurgeons re-examine the case: Neurosurg. 54: 1298, 2004;
and examine a new account Neurosurg. 53: 1019, 2003 -- both articles
highly recommended. Most recent review reaches the one-shooter conclusion:
Plast. Recon. Surg. 132: 1340, 2013.
ABRASIONS result from friction removing the epidermis, with little or no damage to the dermis. They heal with no scar. The pathologist will usually see a remnant of the epidermis at one edge.
Ante-mortem abrasions are reddish from inflammation and perhaps minor bleeding. Post-mortem abrasions are yellow, with a fibrin coating resembling parchment. A good rule is that if a wound has a yellow edge, it is post-mortem (why?) {07064} abrasion
An abrasion may be the only external sign of blunt force injury, which may have done serious internal damage. "Pressure abrasions", from vertical force, are common over the zygoma and the side of the nose and orbits when someone falls. "Patterned abrasions" may tell the nature of the object causing the injury (i.e., tire tracks, pipes, rings on a fist), or merely the clothing. "Nail scratches" need no description; "claw marks" are deeper, U-shaped lesions that have penetrated the upper dermis. * Future pathologists: Here's a system for dating abrasions under the microscope: * And for hard-core pathologists dating skin wounds... (AJFMP 16: 203, 1995)
Always present:
CONTUSIONS are areas of hemorrhage in soft tissue, due to ruptured blood vessels, due to blunt trauma. Same as a "bruise". Usually, we reserve "contusion" / "bruise" for cases in which the overlying skin is not broken. If it's palpable, it's a "hematoma". The blood in most skin bruises is mostly in the subcutaneous tissue. Bruises become more prominent with time, because the blood cells themselves (if they stay intact) and their liberated hemoglobin (if the leak or lyse) spread into the overlying dermis. Like abrasions, contusions may or may not be patterned. A patterned contusion, unlike most others, has most of its red cells in the dermis from the beginning, because the dermis was forced between protuberances on the impacting surface. Some purists say that a bruise is a contusion visible through the skin. It's easier to bruise loose tissue (your orbit) than tightly-woven tissue (your palm). {07065} kid beaten with electric cord
Don't mistake the "mongolian spot" or other pigmentation for a contusion. Remember that bruises show up better on light-skinned people, and that scalp bruises are often hard to see. If in doubt, incise the lesion. Colors of a bruise: Blue/purple --> violet --> green --> yellow --> vanishes. Sadly, the rate of color change is tremendously variable, and you can't use it to estimate the time of a bruise. One recent study (For. Sci. Int. 50(2): 227, 1991) found the only reliable rule is that yellow always means >18 hours. Uh, one of my skydiving bruises showed yellow at 16 1/2 hours. Pretty reliable: If the color has clearly not begun to change, it is less than 48 hours. If the color has obviously changed and become variegated, it is more than 48 hours. Unless there is a hematoma that will organize, histology will usually only show the presence or absence of hemosiderin in the bleed. (Complement isn't going to be fixed, so neutrophils won't be coming in). Hemosiderin, usually not present until 72 hours, may sometimes be present by 24 hours. Even heavy trauma may not produce a bruise. Conversely, bruises can be much larger than the object that produced them, due to stretching and avulsion of nearby vessels. A good rule is that a child who isn't walking shouldn't have a bruise. ("No cruise, no bruise.") After that, a kid living a full, happy life will often have several bruises. Factors making a bruise more severe: NOTE: Yes, you can produce a bruise on a newly-dead body, though with no blood pressure, it won't be as impressive as one produced by the same force in life. And post-mortem extravasation of blood can simulate bruising: AMFJP 19: 46, 1998. * Future pathologists: How to skin a body in search of contusions -- something you'll need to do if the person has died in police or prison custody AJFMP 17: 316, 1996. Advanced decomposition and livor mortis can produce lesions indistinguishable from contusions. LACERATIONS: Splits and tears of skin and/or soft tissue, due to stretching-shearing or crushing, on the body surface or deep inside. 
Don't mistakenly call an incised wound, produced with something sharp, a "laceration". To produce a good laceration, there must be something hard (usually bone) close beneath the point of impact. It's easy to lacerate your scalp or shin, hard to lacerate your abdominal wall. You can spot lacerations by their irregular, crushed, abraded, undermined, bruised edges, and the presence of elastic and connective-tissue bridges in their depths. It's usually (not always) easy to tell these from incised wounds; lesions produced by very dull knives or the edges of boards may produce difficulties. No, the shape of a wound doesn't tell the exact shape of the instrument that produced it. The classic example is the Y-shaped lesion produced by a metal rod. An "avulsion" is a laceration in which a portion of soft tissue has been ripped off the underlying fascia or bone, or an organ ripped off its attachments. The overlying skin may be ripped, or sometimes only a pocket of blood is created deep in the tissues. * Dog bites: J. For. Sci. 38: 726, 1993. The English lady who slept in the hospital with her pet rat that bit her and gave her abscesses: Br. Med. J. 309: 1694, 1994. BLUNT TRAUMA TO THE CHEST {07040} motor vehicle accident
The costal arches provide more protection to older adults, in whom they have usually calcified. Younger people may have organ damage with little external evidence of injury. Ribs fracture because of (1) direct blows over one or more ribs; (2) indirect trauma from front-to-back chest compression (falls from a great height, getting run over, CPR); (3) pathologic fractures (metastatic cancer, primary bone disease); (4) child abuse (especially by today's savvy abuser who knows he/she can "blame the injuries on CPR" -- Am. J. For. Med. Path. 21: 5, 2000).
Problems caused by fractured ribs: Fracture of the sternum usually results from steering wheel injury, people jumping on the chest, getting run over, or CPR injury. Seat belt injuries: J. For. Sci. 38: 972, 1993. You're still better off with it on than with it off. Listen to the safety ads: politicians realize that seat belts save lives, and (of course) money. BLUNT TRAUMA TO THE HEART AND PERICARDIUM
A bruise to the heart may undergo necrosis, produce rhythm and EKG disturbances, and develop an aneurysm just like an acute MI. * The modern police weapon, a beanbag to stun and knock over perpetrators: Ann. Emerg. Med. 38: 383, 2001. A laceration of the heart may produce rupture (free wall, septal, papillary muscle, chorda). The left coronary artery or its plaques may be damaged, or a dissecting hematoma may be produced in the aorta or coronary system. Forcing the heart downward may rip the ascending aorta transversely. This usually happens in steering wheel injuries. Or the sudden compression of the heart may burst the ascending aorta. Or a sudden deceleration injury can lacerate the descending aorta just beyond the origin of the left subclavian artery. (How do you think that might happen?) If the vertebral column is fractured and dislocated, the aorta may be ripped. Tiny rips in the aorta may bleed late, or develop into post-traumatic "pseudo-aneurysms", with their walls composed only of collagen. {03224} "steering wheel" aortic transection
DIAPHRAGM AND LUNGS In addition to the familiar iatrogenic pneumothorax (positive-pressure respirators, needles in the chest), blunt trauma to the chest can rip the tracheo-bronchial tree or the pleura beneath a rib. If the lung is compressed while the glottis is closed, there may be several bursting ruptures of the lungs. TENSION PNEUMOTHORAX results when a bronchus or portion of pleura is ruptured and the airway communicates with the pleura. During inspiration, air is forced into the pleural cavity. During expiration, the flap closes, and air remains in the pleural cavity. Eventually, the mediastinal structures will be shifted away from the tension pneumothorax, compromising venous return to the heart. Rupture of the diaphragm from strong compressive force at or below its level is fairly common, particularly on the left, where the liver affords less protection. Future pathologists: In suspected child abuse, one favorite defense is "the child simply stopped breathing / choked and the injuries resulted from CPR". Each case must be considered individually. In-hospital CPR in kids without bleeding problems doesn't seem to cause retinal hemorrhages, and if they occur at all they're tiny (Pediatrics 99: E3, 1997). Old claims about CPR causing serious liver lacerations (NEJM 207: 500, 1962) reflect the era's ignorance about child abuse. CPR occasionally ruptures the stomach of a child, but beyond this, the injuries it causes children seem minor (Am. J. For. Med. Path. 21: 5 & 307, 2000). ABDOMEN Even when there is no external evidence of trauma to the abdomen, the liver, spleen, or distended stomach or intestine can be lacerated. (The abdominal muscles are much more pliable; empty hollow organs move easily and are very difficult to injure by blunt trauma.) The liver is very commonly lacerated, by virtue of its consistency and placement. Any surfaces may be shattered, depending on the direction of the force. If there's fatty change, it's even easier to lacerate. Blunt-force injuries to the gallbladder and bile ducts are uncommon except in conjunction with liver injury.
|
Most trauma to the pancreas is due to steering-wheel injuries. The result is typically acute autodigestion, and pseudocyst formation and so forth may occur.
The spleen is hard to rupture unless it is enlarged and/or the capsule is fragile (i.e., infectious mono,
malaria![]() ). In these cases, even mild trauma can rupture it.
). In these cases, even mild trauma can rupture it.
The kidneys may be bruised, but rupture is uncommon, and won't occur in isolation. A full bladder is easy to rupture.
Blows to the pregnant uterus (auto accidents, battery, falls) may separate the placenta from the wall, killing the unborn child. Or the fetus may be injured; little is known of the anatomic pathology in this situation.
* Future pathologists: Most "rupture of the distal esophagus / stomach" seen at autopsy occurs early-postmortem as part of putrefaction ("esophagogastromalacia"). Histology shows no vital reaction. Don't be fooled.
* Future pathologists: Trauma to the liver is commonplace as a result of CPR ("oops, a little bit low....") in adults, but in kids this is very uncommon (Am. J. For. Med. Path. 21: 307, 2000).
INJURIES TO THE EXTREMITIES
These most often result from motor vehicle accidents, falls, and battery. Several things are worth remembering.
Fracture of a long bone can produce a fat embolus.
{07145} fat embolus (oil red O, glomerulus)
{07148} fat embolus (brain capillary)
{07149} fat embolus (bone marrow in lung artery)
Crush injuries can result in myoglobinuria and temporary renal shutdown.
OTHER SPECIAL TYPES OF BLUNT WOUNDS
"Defense wounds" (sharp or blunt) on a attack victim are likely to occur on the backs of the hands, wrists, and arms.
You'll learn the various types of bony fractures on your orthopedics rotation.
* More about brain trauma when we do CNS. Yes, diffuse axonal injury can result from being hit on the head by a perpetrator (J. Clin. Path. 45(9): 840, 1992). In one pre-Columbian culture from what is now Peru, about one person in three died of blunt head trauma from interpersonal violence. "Females display more wounds on the posterior of the cranium, while males show more on the anterior" (Am. J. Phys. Anthro. 133: 941, 2007).
|
WOUNDS FROM SHARP THINGS
|

Cranach, "Judith Victorious" |
{07068} sharp-thing wound
Instead of producing lacerations, pointed and sharp things produce:
No, 'tis not so deep as a well, nor so wide as a church door; but 'tis enough, 'twill serve: ask for me tomorrow, and you shall find me a grave man.
-- Shakespeare's Mercutio
|
{07043} stab wound of head
{07072} stab wound {07066} stab wound {07071} stab wound {07131} stab wound {07031} stab wounds {07160} stab wound, knife guard went in {38252} stab wound of chest {38256} stab wound of chest |
 |
![]() Ronald Goldman's
Autopsy
Ronald Goldman's
Autopsy
Text only
Not for young or sensitive viewers
|
|
Most fatal stab wounds are knife homicides. You can distinguish wounds by sharp instruments from
lacerations by:
|
 Murder of Thomas Becket Canterbury, 1170 |
The sharper the knife, the easier it is to penetrate the skin. Once the skin is penetrated, it's very easy to go deeper until bone is hit.
Note that a dull knife will give abraded, bruised margins, and a very dull knife will give jagged, contused margins.
If tremendous force is used, you may see the pattern of the knife guard. If both ends of a stab wound are blunt, the ricasso (i.e., the area near the guard where both edges are dull) or the guard itself actually went in.
Knowledgeable perpetrators twist the knife, once inserted, to allow lungs to collapse and vessels to be opened. This is likely to turn the skin wound into a "V", "L", or "Y".
In the real world, it's impossible to determine the size or shape of a knife from the wounds produced.
If the blade is not completely inserted, the track will be shorter than the blade. If great force is used, the track will be longer than the blade. (Remember that the chest wall can be deformed easily.)
If the blade is not completely inserted, the skin wound may be narrower than the blade. If the knife is not moved straight in and out, the skin wound may be wider than the blade.
The elasticity of the skin may also make the width of the wound a few millimeters wider or narrower than the blade (how?)
|
The shape of any knife wound will be determined mostly by Langer's lines (remember those?) If
the wound is perpendicular to the lines, it will gape. If it is parallel, it will remain slit-like.
Here's a thought question. What are the ways that scissors stab wounds might look? |
 Shakespeare's Antony and Cleopatra |
If the knife has a sharp and a dull edge (most U.S. knives do), one end of the entry wound may be more pointed than the other. In reality, both ends are usually sharp, since the knife usually enters obliquely and cuts as it goes, and in any case, both sides of the actual knife tip are often sharp.
If there are multiple stab wounds, it's easier to make an educated guess about how thick and how long the weapon was.
Future pathologists: Don't probe knife wounds much. You'll make them deeper and learn nothing useful.
You can produce a fatal stab wound with anything sharper than a table fork.
Scissors (open or closed), barbecue forks, Phillips screwdrivers, broken bottles, and arrows (target or hunting) all produce fairly distinctive wound patterns. Arrow wounds in North Dakota: J. For. Sci. 34: 579, 1989; in Georgia J. For. Sci. 34: 691, 1989. Nail gun suicides: AJFMP 11: 282, 1990.
|
|
Some clever perpetrators deliver a single icepick blow into the auditory meatus, hoping the pathologist will miss the entry wound and also decide, "Must be sudden coronary death, we don't need do to the head."
| Much less common are fatal stab wounds that are self-inflicted (even macho-men Mark Antony and Yukio Mishima botched their attempts) or accidental (falls onto pitchforks, fences, or knives in dishwasher racks). |
 "I have done my work ill, friends. O, make an end / of what I have begun." |
Stab wounds kill by involving an important organ.
When the heart is involved, death usually results from hemopericardium and tamponade if the injury to the pericardial sac is small, or hemothorax if it is large.
When the great vessels are involved, death usually results from hemothorax or hemoperitoneum.
When the lungs are involved, death usually results from hemothorax, less often from pneumothorax.
When the gut is perforated, death usually results from peritonitis.
Neck wounds (stab or incised) kill by producing air embolization, asphyxiation, or exsanguination. Death may also be due to compression of neck structures by a large hematoma.
In stab wounds of the brain, the patient often does not lose consciousness, at least immediately.
Fatal hemorrhage from a stab wound of the extremity is rare unless the femoral artery is severed.
{53702} guy with "behavioral disorder"
{53703} knife swallowed by guy in {53702}
INCISED WOUNDS
Injury from something sharp (like a stab wound), broader than it is deep (in contrast to a stab wound). A "slash".
 Chinatown |
A person may commit suicide by severing an artery, broken glass may cut the neck, or a neck wound inflicted by a perpetrator may be fatal. (In neck wounds, death is likely to result from air embolism.) A drunkard or druggie may die after punching out a pane of glass. Other incised wounds are very rarely fatal.
Future medical examiners: (1) "Hesitation marks" are very superficial cuts made by the wound-be suicide, prior to making the fatal deep cut. They are generally present if it's a suicide. However, perpetrators may also hesitate or taunt. (2) Would-be suicides seldom shoot, cut or stab themselves through clothing. (3) Perpetrators and would-be suicides will use their dominant hand and locate their cuts accordingly. (4) You'll see "defense wounds" on the palms (grabbed the knife), the backs and ulnar aspects of the arms, and sometimes the legs. (5) Homicidal incisions of the neck are usually long and deep if inflicted from the rear, short if inflicted from the front. (6) In a badly decomposed body, surgical scars may re-open, simulating knife wounds (J. For. Sci. 54: 1152, 2009).
{07398} throat was cut
{07399} hesitation wounds
Most incised wounds have very shallow ends. A "wrinkle wound" is several discontinuous incised wounds, caused when a knife wrinkles the skin, cutting only the crests.
{07383} wrinkle wound
The dimensions of an incised wound tell you nothing about the weapon with which it was made. Again, Langer's lines determine whether the wound will gap. (NOTE: "Gap" is a real verb, cognate to "gape".)
CHOP WOUNDS are categorized separately because they combine features of incised wounds and lacerations, or may appear intermediate.
Machete, meat-cleaver, and propeller wounds belong in this category.
Typically, a chop wound will produce an obvious defect in the underlying bone. Depending on how sharp the instrument is, the overlying wound may appear to be an incision or a laceration.
* How the pathologists approached one of the Jeffrey Dahmer murders: J. For. Sci. 38: 985, 1993.
* A young adult Neanderthal survives sharp trauma to the skull 36,000 years ago: Proc. Nat. Acad. Sci. 99: 6444, 2002.
![]() Sword Wound of Skull
Sword Wound of Skull
NIH Historic Collection
Wikimedia Commons
|
LACK OF AIR: {07045} suffocation
|
ENTRAPMENT AND ENVIRONMENTAL SUFFOCATION
Suffocation is usually accidental, from entering or being trapped where there's too little oxygen (i.e., in a high, un-pressurized airplane, in a fire, in a long-closed rusted-out tank, or deep in a mine with saprophytes and methane) or insufficient air flow (i.e., as oxygen is depleted by the victim, death results; typical case is a kid in an abandoned refrigerator).
Citations of "fatally low percentages of oxygen in the air" recall the hemoglobin-oxygen dissociation curve. Below around 60 torr, the hemoglobin thinks it's supposed to give up oxygen, not take it on board.
At autopsy, you'll find nothing specific.
* Africa's Lake Nyos and other volcanic killer lakes emit carbon dioxide episodically, with mass deaths: J. Forensic Sci. 33: 899, 1988, Br. Med. J.298: 1437, 1989; Sci. Am. 283: 92, July 2001, Nature 409: 554, 2001.
* Relatively common today, thanks to some books promoting it, is suicide by helium or some other inert gas, used to flush oxygen from a plastic bag over the head. Am. J. For. Med. Path. 24: 306, 2003.
SMOTHERING
Death from occlusion of the mouth and nose by something pressing on the face or (less often) something else occluding the airway above the level of the epiglottis.
Smothered homicide victims are the very old, the very young, the very sick, or the very intoxicated. The preferred instrument is the pillow or wet washcloth, or the face may be pushed into the bedding. Or the nose and mouth may be occluded using the hands. For the very debilitated, a wet washcloth is sufficient. The most you will see at autopsy are petechiae (sclerae, conjunctivae), nail marks, and bruising of the lips. Even these will probably be absent.
Positional asphyxia simply due to bedrails is well-known (Lancet 363: 343, 2004). Having the bedrails up might help against lawsuits, but also means that patients who climb over them (to go to the bathroom or for whatever reason) are much more likely to fall and to fall farther. (I'm a sleeping-bag man myself....) Much more on killer bedrails -- Am. J. For. Med. Path. 30: 256, 2009.
{12354} smothered?
![]() Mechanical asphyxia
Mechanical asphyxia
Conjunctival petechiae
WebPath Photo
Less often, homicidal smothering results from inept use of gags by perpetrators. Usually, the victims are elderly robbery victims.
Suicides favor the types of plastic bags from the dry cleaner's; this is very common especially among older folks (J. For. Sci. 56: 810, 2011). "Hemlock Society" suicides favor oral overdosage on a Mexican benzodiazepine followed by placing a plastic bag over the face. Inhaling hydrogen sulfide as a means of suicide has become popular thanks to the internet (Am. J. For. Med. Path. 34: 23, 2013.
As you would expect, where there is no struggle for breath, there will be no petechiae (AJFMP 17: 308, 1996).
In children, death due to smothering by a plastic bag is a common accident. If a mattress is too small for the crib, the child can smother in the gap between them.
* As a pathology resident and afterwards, your lecturer claimed, contrary to classic teaching, that a child or passed-out drunkard or druggie can smother on bedclothes or a mattress. We now know that this is one of the major causes of "SIDS" ("unexpected death of an infant in an unsafe sleep environment"). More later.
Whether the death is homicidal, suicidal, or accidental, autopsy findings will usually be entirely negative.
CHOKING
Obstruction within the air passages. When "natural", the cause is epiglottitis. Your lecturer has seen accidental deaths due to a roll of sliced ham ("just popped it in..."), a section of canned peach, a swollen tongue chewed during DT's, and a set of dentures.
Homicidal choking usually results either from (1) stuffing a baby's mouth with toilet paper to stop its crying, or (2) using a rag in the mouth in conjunction with a gag.
Most deaths from choking are accidents. Common objects in kids include peanuts, un-popped popcorn kernels, little balls and screws, and the caps of ball-point pens. In grown-ups, the "café coronary" usually results from a drunkard swallowing poorly-chewed beef "down the wrong throat". Less often, pills can end up in the airway, or falling into deep sawdust, grain elevators, etc., can cause death.
{07213} candy corn occluding airway
Be careful making this diagnosis, since agonally, perhaps 25% of people get food on the airway, and there can be reflux when the dead body is moved.
| Drunkards, druggies, and the very debilitated can and do die of aspirating chewed food or vomit. |
 Jimi Hendrix |
Don't accept "laryngospasm" as a cause of death. The larynx would relax when hypoxia becomes severe.
However, classic textbooks of forensic pathology give little play to airway obstruction in unconscious or very debilitated patients due to the tongue. Ask any anesthesiologist; this is important, and probably is the final pathway out of life for many people.
MECHANICAL ASPHYXIA
|
Pressure outside the body can also cause asphyxia. Familiar causes include large snakes (J. For. Sci. 34: 239, 1989), riot crush, falling into grain (kills a few dozen agricultural workers each year), garage doors (kids playing with the automatic opener: Ped. 98: 770, 1996), human piles, and cars falling off the jack onto your chest. Each time you breathe out, your chest is further constricted. When you try to breathe back in, you cannot. |
|
At autopsy, you'll see bruises, petechiae all over the conjunctiva and sclera, and impressive congestion of the head. (* Future medical examiners: Lots of things can give you petechiae on the eyes by producing strong pressure waves. See, for example, J. For. Sci. 38: 203, 1993).
An important variation is POSITIONAL ASPHYXIA. Someone may slip into a confined space, and each exhalation causes the person to slip deeper. Or a person may lose consciousness with the neck flexed or in some other position so as to compromise respiration ("positional / postural asphyxia"; see Am. J. For. Med. Path. 32: 31, 2011).

|

|
STRANGULATION: Occlusion of the blood flow and/or air passages in the neck by external compression. (If there is a contribution from body weight, it is considered hanging rather than strangulation).
In any strangulation, death is due to lack of oxygen to the brain. While the carotids are easy to compress, it takes severe twisting of the neck to occlude the vertebral arteries. Nothing you can do will occlude Batson's plexus, which is an important part of the venous drainage of the brain.
In hangings, the pressure is often great enough to prevent most arterial flow to the head, and therefore, you will probably not see petechiae, and being vertical makes drainage by Batson's plexus easy. In fatal ligature and manual strangulation (and often but not always in smotherings), there will always be petechiae on the conjunctivae. The finding is by no means specific; you can see petechiae here in death from right-sided heart failure, after vomiting, or even from lying face-down after death.
* Popular ideas about strangling, including what you may see in the movies, are influenced by what is deservedly the most famous depiction onstage. Shakespeare's Desdemona is strangled / smothered by her husband and left for dead. Emilia comes in. Desdemona revives briefly, speaks, then dies. Either this is Shakespeare's poetic license (seems most likely) or she was rendered unconscious by occlusion of the mouth-and-nose, trachea, and/or carotids, then revived, succumbing moments later to increasing edema of the tongue-throat or larynx from injury during the struggle. This probably doesn't happen in real life. Alternatively, the director can have Othello stab Desdemona to death in front of Emilia. This is much more medically accurate, and has been done with much impact.
|
{07056} petechiae in strangulation
{07074} manual strangulation |
It's difficult to occlude the airway by compressing the neck. If this is done, it's done by pushing up on the larynx and hyoid to occlude the back of the throat.
* The Whitechapel serial killer ("Jack the Ripper") was neither the first nor the last serial killer of prostitutes, but was the first to gain a great deal of media attention. When the woman lifted her skirts and thus had both hands occupied, the killer strangled her, probably pushing the larynx up or compressing it from both sides in order to prevent a loud cry. He then laid the body down gently on the ground, turned the head to the left, stood on the right side, and cut the left side of the throat to prevent blood from squirting onto himself. Like others of his kind, he took anatomic souvenirs. He did not have sex with, or masturbate over, the bodies. Probably we will never find out who "Jack the Ripper" actually was.
* Sphincter incontinence is common in strangulation, but by no means inevitable. Erection and ejaculation during judicial hanging are probably legends.
* Suicide by self-strangulation is probably not going to work, playing the "choking game" at home can kill you accidentally, and one can render onesself unconscious while carrying out a complex suicide (J. For. Leg. Med. 18: 336, 2011 -- self-strangulation on the ledge of the 13th floor, caught on a mobile video).
HANGING: Compression of neck structures is secondary to a noose tightened by body weight. Review of the anatomy: Forens. Sci. Int. 56: 65, 1992.
Most of these are suicides or accidents in folks doing autoerotic self-entertainment; children may hang themselves accidentally (J. For. Sci. 55: 637, 2010). The weight of the head (12 lb) slightly exceeds the weight required to compress the carotids. The victim may be fully suspended ("complete hanging"), or upright with legs on the floor, kneeling, sitting, or lying down ("partial hanging", but just as dead). It takes 33 lb of pressure to compress an adult's trachea, so this usually doesn't happen in a hanging. Sometimes, death is due to the tongue being forced upward to occlude the airway.
* Now that so many people are filming their autoerotic escapades and suicides, we have the time sequence well-documented. Unconsciousness in 10+3 seconds, then as you'd expect seizures, decerebrate rigidity, decorticate rigidity, loss of muscle tone, loss of respiratory movements, and last muscle movement in 3-7 minutes. Am. J. For. Med. Path. 32: 104, 2011.
* Homicidal hanging, i.e., the victim was very drunk or drugged up or was rendered unconscious by a blow to the head, requires an alert police officer and/or good pathologist: Med. Sci. Law. 50: 224, 2010.
You'll usually find the noose above the larynx. Look for marks, unless the ligature is soft and the body was taken down soon after death.
After most hangings, you'll see a protruding tongue. Don't expect always to see deep injuries in the neck, or petechiae around the eyes (why not?) Muscle injuries are common; maybe 2/3 have a bleed (grade I strain) at the clavicular origin of the sternocleidomastoid from the stretch (Am. J. For. Med. Path. 33: 124, 2012).
A murderer may kill or disable someone and hang the body afterwards to simulate a suicide, perhaps even typing the suicide note onto Facebook like people do nowadays. One of the really tough calls in forensics is strangling someone and then suspending the body. In a real hanging, the hyoid and especially the cricoid are unlikely to be damaged as they are in a strangulation (Am. J. For. Med. Path. 33: 4, 2012.)
TARDIEU SPOTS are small hemorrhages resulting from the weight of a column of blood rupturing blood vessels after death. These can be impressive in the lower extremities of a hanged body.
{07046} hanging
|
In JUDICIAL HANGING, the "client's" upper cervical vertebrae (C2, C3, and/or C4) are supposed to be broken and/or dislocated by a carefully-planned drop (* actually, doing this right is the exception: For. Sci. Int. 54: 81, 1992). The classic "hangman's fracture" is through the pedicles of C2, with hyperextension of the neck pushing C1 and the body of C2 into the spinal cord, causing instant death. Suicides won't be able to do this unless they have cancer, Down's (maybe), rheumatoid arthritis, or osteoporosis weakening the vertebral column. |
 Goya, "Hard is the Way" |
|
|
|
|
![]() Hanging of Jewish civilians
Hanging of Jewish civilians
Romania under Nazi occupation
WWII era
SEXUAL (AUTOEROTIC) ASPHYXIA: A curious, fairly common accident in which a man hangs himself while acting out his personal, private, kind-of-unusual sexual fantasies.
There are may be 500-1000 of these deaths each year in the USA (Am. J. For. Med. Path. 33: 143, 2012). You are likely to find (1) a towel or cloth between the rope and the neck, to avoid producing a hard-to-explain mark afterwards; (2) dirty books and pictures, women's clothing, a mirror, and/or maybe even a camera; (3) some kind of evidence that this isn't the first time (i.e., check that closet top for rope marks); (4) something to prevent his semen from splattering; (5) the deceased could have tied himself up that way. Review AJFMP 16: 232, 1995.
Don't try to understand it. Your lecturer doesn't believe these men do this stuff "because hypoxia heightens orgasm". If this were true, more men would ask their wives and girlfriends to squeeze their necks during romantic interludes. Being tied up is a well-known turn-on for lots of men, alone or with their special partners. Danger may also be a thrill (I wouldn't know, skydiving is very safe). Guys: if you do this stuff, just don't tie the rope around your neck when you're alone.
* Different things are turn-ons for different men, and some men inhale icky things rather than tying
themselves up. Your lecturer autopsied one 15-year-old who died from inhaling "Pam" pan spray while
masturbating. These are all accidents, not suicides. Two different guys and their accidentally-fatal
romantic relationships
with
their hydraulic tractor shovels: J. For. Sci. 38: 359, 1993. Also Psych. Clin. N.A. 15: 703, 1992
("the dangerous paraphilias", enough to make it obvious enough that it's the link with physical danger that's a
turn-on).
* Once considered a "men-only" phenomenon, we now know that a few women do this stuff, too.
The difference is that women almost never use props, toys, or funny clothes (For. Sci. Int. 48: 113,
1990).
![]() Autoerotic asphyxia
Autoerotic asphyxia
Source unknown
Not for young or sensitive visitors.
Hanging is a very popular method of suicide for teenaged boys (i.e., it works, it takes little planning, and they are less likely to have firearms than grown men). Both teens and pre-teens can die accidentally doing the "choking game" in the schoolyard or alone at home.
Homicidal hanging is rare, but a very clever perpetrator who is alone with the victim in a private place can render the victim unconscious by a blow to the head and then hang him. The subgaleal hematoma will be the giveaway. Authentic-looking noose marks can be made on a body if it is hanged two hours or less after being murdered by some other means. When in doubt, a complete autopsy is worthwhile.
* Grammarians: People are "hanged", inanimate things are "hung". The only exception is when a man is bragging (or, less likely, getting a compliment) about his equipment.
Many a good hanging prevents a bad marriage.
-- Shakespeare, "Twelfth Night"
LIGATURE STRANGULATION: Compression of neck structures is secondary to a noose tightened by something other than body weight
|
These are usually homicides, and the victims are usually women. An occasional enterprising suicide may use a tourniquet method, and lie on the stick to hold it in place (Am. J. For. Med. Path. 30: 369, 2009; Am. J. For. Med. Path. 31: 85, 2010). Accidental ligature strangulations occur (for example, Isadora Duncan's scarf, some skydiving mishaps). |

|
The appearance of the mark can be highly variable. If a towel is used, there may be none. Future pathologists: Don't mistake ordinary crease marks of newborns, folks with jowls, or decomposed people for ligature marks.
Again, expect to see conjunctival petechiae.
|
{07189} ligature strangulation
|
 Goya, Interrogation by Mock-Strangulation |
MANUAL STRANGULATION: Compression of neck structures by someone else's body part.
This is always homicidal. You can't strangle yourself. (Possible exception: Someone bumps his own carotid sinus and has a rhythm disturbance. I think this is very unlikely unless the person is already very sick. Anyway, this hardly counts as "manual strangulation".)
There will always be conjunctival petechiae. Usually, the force used is sufficient to produce hemorrhage. Older people tend to have more extensively calcified (and therefore breakable) thyroid cartilage horns, hyoid bones, and tracheas. Ante-mortem fractures of the hyoid bone are pathognomonic of manual strangulation (unless there's another obvious reason, of course -- Med. Sci. Law. 51: 109, 2011). As usual, there must be hemorrhage, or you can't call a fracture ante-mortem.
Again, look for nail marks ("claw marks", "scratch marks"), little bruises, and so forth. "Clever" perpetrators strangle drunkards and children using the palm, without producing finger marks or damaging the deep structures of the neck. In this case, there may be no marks.
 |
* Medical historians! Burke and Hare, old-time Scottish medical school anatomy department provisioners, decided that robbing new graves was too much work. They started obtaining the corpses of poor folks by "burking", i.e., sitting on the chest and occluding nose and mouth with their palms. |  |
{07047} strangled by hand
{07137} strangled by hand
![]() Strangled by hand
Strangled by hand
Ed Lulo's Pathology Gallery
* Future pathologists: If you suspect strangulation, open the head before you dissect the neck. This will prevent overdistended veins, especially between esophagus and spine, from rupturing and confusing the picture.
Future criminal-justice types: CHOKE HOLDS (really, "bar arm holds") may produce death by (1) fracturing the airway, (2) hypoxia sensitizing the heart to rhythm disturbances induced by catecholamines during the continuing struggle, or (3) atheroembolization. CAROTID SLEEPER HOLDS compress the carotids only, but as the recipient struggles, the neck can be damaged.
Future medical examiners: Blood behind the esophagus, or next to the cervical spine, or petechiae on the laryngeal and epiglottis mucosa mean nothing. Don't send somebody to jail for a non-strangling.
The popular defense theory, "He just bumped her neck over the carotic sinus and the cardioinhibitory reflex killed her" is pretty far-fetched but just possible. It depends on the expert (Am. J. For. Med. Path. 33: 8, 2012.)
* Future criminal defense attorneys: If I'm the pathologist, please don't allege that your defendant and the victim were merely "playing the choking game" or that "he just happened to bump her carotid sinus" or "it was rough sex" or "he was just giving her a neck massage". The last worked for iconic Marxist philosopher Louis Althusser after he strangled his wife. Althusser was a "famous intellectual" -- he coined and popularized the term "antihumanism", and "unified psychoanalysis and Marxism" with an "explanation" of why people's inner neuroses keep them from accepting the obvious glories of Communism. As such, he was sure he know how the rest of us should live our lives and how the world should be governed. Be this as it may, the judge found he was too nutty to stand trial and put him in away in a psychiatric hospital.
CHEMICAL ASPHYXIA
Hydrogen cyanide, carbon monoxide, and hydrogen sulfide (oil refineries, manure pits, geothermal plants) are poison gases.
CYANIDE (JFMP 18: 185, 1997; Am. J. For. Med. Path. 23: 315, 2002): Blocks the cytochrome system.
Cyanide sodium and potassium salts are used in electroplating, as fumigants, and as insecticides. There is marked dyspnea before death, and criminals in the gas chamber have signalled that death from cyanide gas is, indeed, painful.
* Burning plastics produces cyanide, and often people who die in household fires have lethal levels of cyanide in their blood. This is always a consideration in treating people who have been in house fires, as is carbon monoxide (Clni. Tox. 50: 759, 2012).
Unlike in the spy movies, it always takes a few minutes to die of cyanide poisoning, even when it is in gas form, and victims remain conscious for a while. (This happened in the Nazi death camps, and in the gas chambers used for capital punishment.) You need around a fifth of a gram of either the salt or the gas; when the salt is ingested, stomach acid (if present) turns it into the lethal gas. (* NOTE: Rasputin probably had achlorhydria; why?)
At autopsy, look for (1) bright red blood (i.e., cyanide prevents utilization of oxygen) (2) the "bitter almonds" smell (around 1 person in 3 cannot smell it; I cannot); (3) thiocyanate in the blood (normal folks, especially smokers, will have some of this on board already.)
We know of no cumulative harmful effect from cyanide.
* Politics and junk science.... The FDA banned Chilean grapes in the early 1990's. Someone analyzed exactly two grapes (really!) and discovered traces of cyanide in both. What the media didn't tell you, and the FDA apparently didn't know or care, is that there's a small amount of cyanide (as nitrile) in all grapes, and that there was no more cyanide in the grapes in question than in any other grapes. I am not making this up. The result was a major public scare, and an economic disaster for the poor people of Chile. See Nature 369: 27, 1994.
CARBON MONOXIDE (AJFMP 18: 406, 1997; NEJM 360: 1217, 2009).
The colorless, odorless, slightly-lighter-than-air gas (why firemen may crawl at a fire scene) that results from burning carbon in relatively
low amounts of oxygen. House fires, defective home heaters, and old-fashioned lamps and generators
used during natural disasters (Pub. Health Rep. 126-S1: 108, 2011)
are the common sources. Before the era of the catalytic converter,
automobile exhaust contained about 5% carbon monoxide. The stuff has a much greater affinity for heme than
oxygen does, and the concentration in the atmosphere need not be high to cause trouble.
(People have died from being placed near the exhaust pipes of ambulances prior to transport).
There's
plenty in cigaret![]() smoke.
smoke.
Carbon monoxide acts in part by tying up hemoglobin. Its affinity for hemoglobin is 200 times that of oxygen. Smokers are likely to have 10% saturation of hemoglobin. Saturation from 20-30% will make you sick (it's at this point that cherry-red lividity may appear). Saturation of 60% or more will probably kill you (less if you've got angina, emphysema, etc.)
Obviously this isn't the whole story, because the symptoms of carbon monoxide poisoning are not the symptoms of anemia. There are a host of other mechanisms as well. The damage to the cytochromes, endothelium, and lipid membranes are being worked out.
In ACUTE TOXICITY, there is headache, drowsiness, loss muscle strength (carboxymyoglobin) and ultimately confusion and coma.
The pathologist will find cherry-red livor-mortis, but this isn't specific. You can see it in hypothermia, or cyanide poisoning (or the biochemistry-class fluoroacetate poisoning) as well. Fortunately, there are instruments to measure the amount of carbon monoxide in the blood.
After an episode of acute poisoning, there may be residual difficulty with memory, speech, and/or coordination. If the patient survives for four or more days, necrosis of the globus pallidus is common. Occasionally, the damage to the globus pallidus is not apparent, and the patient seems to recover, but then goes on to develop progressive destruction of the globus over months, by some unknown mechanism (Brain 134: 3632, 2011).
* Now that cars produce very little carbon monoxide, successful garage suicides are much less common, and usually result from oxygen depletion and carbon dioxide overload rather than carbon monoxide, though some will be produced when the oxygen in the air is relatively depleted (Am. J. For. Med. Path. 23: 123, 2002).
{07013} carbon monoxide, acute; note the cherry-red livor mortis
{07116} carbon monoxide after-effects on globus pallidus
![]() Carbon monoxide
Carbon monoxide
Cherry red
WebPath Photo
In CHRONIC TOXICITY (i.e., that home heater is defective), the family complains of headache and malaise. Since carbon monoxide accumulates over time, symptoms do not vanish simply from leaving the house. It takes a clever physician to make the diagnosis, and ultimately save the family from brain damage / death.
|
{24922} burn
{46535} burn {46536} burn |
|

| Nanking, 1937 |
SURFACE BURNS
FIRST DEGREE: The outer epidermis is damaged. The dermal vessels probably dilate, but there are no blisters.
SECOND DEGREE: Living cells are killed in the epidermis. There will be a blister.
THIRD DEGREE: No more epidermis.
FOURTH DEGREE: Charred through.
Today, it's more meaningful to talk about PARTIAL THICKNESS and FULL THICKNESS burns. In the latter, all the skin adnexal structures (hair follicles, sweat glands) are gone from the region of the burn, meaning you will need a skin graft to re-epithelialize it.
![]() Fatal burns, "necklacing"
Fatal burns, "necklacing"
African political punishment
Burning tire is placed around neck
You'll learn the "rule of 9's" for estimating surface area burned. Complications of burns include:
* By contrast, violence against women in Pakistan and Bangladesh is often carried out by means of acid-throwing -- Pakistan outlawed the practice in 2010 (Lancet 376: 1209, 2010).
{07186} thermal injuries
{07103} second-degree burn histology
{07184} could be Curling's ulcers
INTERNAL THERMAL INJURIES
House fire temperature is usually around 1200F, and this isn't nearly hot enough to ash a body. Typically, people dying in house fires are found more or less blackened, and often in the "pugilistic attitude" (i.e., like a boxer) with the strongest muscles flexed.
People caught in a burning building inhale smoke, fumes, and heat. Often (and mercifully), the immediate cause of death is hypoxia and/or inhalation of carbon monoxide and/or hydrogen cyanide.
Damaged lung will develop ARDS, pneumonia, and so forth. Histopathology of lung lesions following household fires: Hum. Path. 21(12): 1212, 1990 (there are few surprises).
Persons dying in fires typically have soot in the airways, and will always have elevated carboxyhemoglobin levels. (Arson is a time-honored means of trying to conceal homicide. A murder victim whose trailer is then burned by the perpetrator will not have soot in the airway or much carboxyhemoglobin on board.)
The medical examiner can usually make an identification of the body by means of dental records or fingerprints.
* In a flash fire, there may be instantaneous edema of the oropharynx and glottis, preventing entry of soot into the trachea or carbon monoxide into the blood (AJFMP 17: 24, 1996). My own worst mistake in pathology resulted from my not knowing this. * Chemical burns due to attempted theft of anhydrous ammonia from farm tanks by methamphetamine-manufacturers have become commonplace.
* SPONTANEOUS HUMAN COMBUSTION is a myth. In the best-documented cases, the
deceased is an overweight alcoholic who has passed out while smoking in a big cottony chair. The
ashes fall, the chair smolders, the victim is overcome by carbon monoxide, the fat melts, and the
"candle effect" (fat moves up the clothing like wax up a wick)
reduces the cigaret![]() ,
chair and victim to ashes without burning down the house.
When the body is found, the pathologist should call it "isolated body
combustion".
,
chair and victim to ashes without burning down the house.
When the body is found, the pathologist should call it "isolated body
combustion".
NOTE: Please don't smoke in bed, even if you are drunk.
DROWNING (Am. J. For. Med. Path. 27: 20, 2006 deals with children but is just as applicable to adults; NEJM 366: 2012, 2012.)
Definitions:
If you are rescued, it's "non-fatal drowning." If you die of it before or after being rescued, it's "fatal drowning." There is no longer any such thing as "near-drowning", "wet / dry drowning", "delayed onset of respiratory distress due to near-drowning", etc., etc.
Probably more material of a speculative nature has been written about drowning ("fresh water vs. salt water"; "electrolytes in the different cardiac chambers"; "wet versus dry drowning", "finding diatoms" -- Med. Sci. Law. 51-S1: S7, 2011 -- , etc.) than about any other subject in pathology. The reason, of course, is the problems with determining whether a dead body was alive or dead when it entered the water. Don't worry about this stuff.
| In drowning, death is generally due to asphyxia. If water enters the lung (occasionally, laryngospasm prevents this but it is probably rare -- AJFMP 25: 291, 2004), expect to see foam in the mouth. Even a little bit of hypotonic or hypertonic water in the lungs wrecks havoc on the alveolar membranes, so the fluid in the lungs is likely to be blood-tinged. A pathologist's essay on handling bodies from the water: J. Clin. Path. 45(8): 654, 1992. |

Shakespeare's Ophelia |
* Many freshly-dead bodies float in fresh water, and a majority in salt water. Pushing the body below the surface forces air from the lungs and generally will make the body sink. Unless the body is very well weighted-down, it will eventually float back to the surface due to gases of decomposition.
When a child "drowns in the bathtub", look for other evidence of child abuse (Arch. Ped. Adol. Med. 150: 298, 1996; Ann. Emerg. Med. 25: 344, 1995; Arch. Dis. Child. 70: 435, 1994) -- holding a child under the bathwater is a fairly common form of child abuse, and when fatal, it may be unusually difficult to prove.
* Drownings during "water birthing", a "pop"/"holistic" practice that is widespread in Europe: Am. J. For. Med. Path. 31: 258, 2010).
* Future pathologists: In fresh-water drowning with rapid death, the systemic arterial blood will be hypotonic, the red cells likely to burst, and their hemoglobin to stain the aortic intima (but of course sparing the pulmonary artery's intima. See J. Clin. Forensic Med. 13: 125, 2006. Hyponatremia of the blood in the pulmonary venous return stops the effective beating of the left ventricle.
* You remember that people with the long-QT mutations KCNQ1 or RyR2 are prone to die suddenly when they jump into water (Mayo Clin. Proc. 80: 596, 2005 for the molecular autopsy). Something about the "diving reflex".
Near-drowning, of course, is a serious cause of brain damage (Emerg. Med. Clin. N.A. 10: 339, 1992; there is a self-help group for friends of these unfortunates in Kansas City).
"Drowning is a diagnosis of exclusion." The impossibility of making this diagnosis on decomposed remains was showcased at the Casey Anthony trial fiasco in 2011, and almost certain explains the (to me, surprising) acquittal.
* "Immersion syndrome" is the sudden death of a healthy swimmer immediately after immersion in cool or cold water, with a negative autopsy. ("Diving reflex", anyone?) In addition to the infamous long QT channelopathy, other causes are alleged -- this is supposed to be one of the toughest calls in forensic pathology (J. R. Army Med. Corps 151: 250, 2005. The folks at Mayo's, who test for channelopathies, report a high incidence of the ones that cause sudden death on jumping into water in an (admittedly selection-biased) series of folks who drowned unexpectedly (Mayo Clin. Proc. 86: 941, 2011).
Bodies found in the water are likely to have a variety of injuries from being in the water, including scrapes, bumps, and lesions attributable to amphipods (little-known but ubiquitous crustaceans -- see For. Sci. Int. 209: e16, 2011 and For. Sci. Int. 212: e18, 2011.)
* I am not aware of any reason to think that swimming is more dangerous after eating. An odd paper in Med. Sci. Law. 51: 161, 2011 merely suggests to me that people who intentionally drown themselves are less likely to have a nice meal beforehand.
* Future scene investigators: In an alleged "accidental bathtub drowning", look for other injuries on the body, and splashed water.
{07139} drowned; the foam is a mix of pond
water and lung surfactant
{07147} drowned
{07027} decomposition speeded
by warm water
PRESSURE CHANGES
BLAST INJURIES
Air blasts are actually high-amplitude sound waves emanating from explosions. The blast can enter and blow out the lungs and their vessels, or compress the chest, or rupture hollow organs in the abdomen. The physics is easy to understand: Body parts with different densities will be displaced relative to one another, causing them to be torn.
In immersion blast, the same physics applies. Under these circumstances, it's best to be floating prone or supine on the water surface. Guess where the water blast goes if you're treading water.... The bowel is the body-part most likely to be injured.
Bomb and land mine injuries combine projectiles and blast force. As long as the US, Russia, and China are all still manufacturing land mines, the prospects for their elimination seem poor (Lancet 357: 731, 2001).
DECOMPRESSION INJURIES ("caisson disease", "the bends"; Lancet 377: 153, 2011)
When the pressure of a person's surroundings decreases greatly, dissolved gas in the blood and tissues will turn into fine bubbles, wrecking havoc (primarily by plugging the microvasculature; in science-fiction it includes bursting-apart of the body though this did not happen to the Russians whose space capsule decompressed). This happens in real life when divers surface too rapidly, or in futuristic fiction, when spacemen remove their spacesuits at the wrong time.
This is quite unlike the more familiar air emboli, since the masses of foam in the blood are much harder to push through the small vessels (compressability, surface tension).
ELECTRICAL INJURIES
Low-voltage alternating current (i.e., 110 volt household current) kills by inducing ventricular fibrillation; or if the amperage is high, the heart simply cannot re-polarize. C=V/R, where: C is current in amperes
|
 |
Effect of current:They finger death at their gloves' end where they piece and repiece the living wires.
-- Rudyard Kipling, "The Sons of Martha"
 |
Electrical burns are generally small, gray, charred marks with a grayish-white rim (blood was driven
out, then vessels were seared closed). And in the large majority of electrocutions
on household appliances, there is NO lesion found on autopsy.
|
Lightning is direct current, and thus produces a different kind of injury (review J. For. Sci. 38: 353, 1993). The typical lightning stroke produces arborescent (fern-shaped "Lichtenberg figures") burns. They are distinctive (review AJFMP 17: 99, 1996 -- future pathologists, they are best seen at the death scene and may fade). The cell membranes are damaged by current rather than heat. If the lightning passes through heart or brainstem, the victim is likely to die. Otherwise, survival is usual, and injuries may be mild or severe. Around 1/3 of people struck by lightning die. All about being struck by lightning: AMFJP 17: 89, 1996. Remember it does not have to be raining or even cloudy ("bolt from the blue") for there to be a lightning strike, especially on a hot day.
* My physicist friend Konrad Grygorczyk explained to me: "All electrical injuries, whether A/C or D/C, should look like Lichtenberg figures if you could see a snapshot of them as they happen. Burn marks can serve as that snap shot only in the case of an intense, short burst of electricity. Since the path of conduction is constantly changing, a weaker burst will produce burns only in places exposed to sufficient current over longer intervals. So burns that take longer to happen reflect an average path of greatest current intensity rather than a snapshot. So the different patterns reflect differences in timing. In general, electrical conduction is stabilized by an effect called self-inductance which acts to dampen any sudden changes. Since lightning is an auto-catalytic process it can overwhelm even that natural stabilizing effect. As soon as there is tiny current making its way to the ground, it cascades into huge bursts."
![]() Struck by lightning
Struck by lightning
Lichtenberg figures
Patient photo from NEJM
If you're outside in a storm and your hair starts to stand up and you feel tingly, lightning is about to strike. If you can't get in a car, get to the lowest ground that you can and crouch ("catcher's position)". This is the new advice from the National Weather Service, which is concerned about your heart being close to the ground, which carries current for a few hundred feet, should you lie flat. No controlled studies are posible, and since so far as tasers seldom cause a cardiac rhythm problem (supported in J. For. Legal Med. 17: 1, 2010), this sounds hokey to me. Any physicists out there?)
* {07519} ...and that one word were "Lightning!", I would speak.... -- Lord Byron
 {07190} lightning wound
{07190} lightning wound
{07513} lightning wound
{07037} electrical injury and burn
{07107} electrical trauma
{07109} lightning death
{07504} lightning death
{07183} electrocuted
{07187} electrical injuries
{07480} electrical injuries
{07486} electrical injuries
{07495} electrical injury, where current exited
{11127} electrical injury, where current exited
{07537} lamp-in-the-bathtub homicide
| * A judicial execution uses 31 cents worth of electricity (1990 figure). In reading up on the history of judicial electrocution in the U.S., I learned that it's easy to bungle, but probably nobody has suffered since Thomas Edison's foolish attempt to electrocute a criminal by running a current from one arm to the other (!). |
 Electric chair at Sing Sing |
Under given circumstances that surfaced, the results were far less than aesthetically attractive. But with rare serene exceptions, after forty-odd years of experience, it is held that most deaths are without aesthetic attractiveness, regardless of causation.
-- Frank Kilgo, M.D.;
Medical Director, Florida State Prison, after a condemned man accidentally caught on fire in the electric chair
HEAT EXHAUSTION AND HEAT STROKE ("hyperthermia")
These result from over-production of heat, or the inability of the body to radiate heat. Babies, the elderly, and those taking anticholinergic agents and phenothiazine drugs are especially vulnerable to these problems.
In HEAT EXHAUSTION, a person over-exerts in a hot environment. As a result, fluid and electrolyte imbalances and lactic acidosis may render a person sick or even dead. In addition, the over-exertion can result in rhabdomyolysis and myoglobinuria.
In HEAT STROKE, the body temperature rises, by whatever means, to a point at which the brain no longer properly controls body temperature (around 41C or 106F). The result is rapid, generalized vasodilatation, coma, and death.
Classic textbooks make a big distinction between "heat exhaustion" and "heat stroke", but in practice, it's likely to blur. Scenarios range from forced exercise on a hot day, to forced labor in hot quarters, to cocaine abuse, to extreme fever.
* My friend Barry Lifschultz MD, medical examiner in Chicago, was one of the authors of the epidemiologist's criteria for a heat-related death (Am. J. For. Med. Path. 18: 11, 1997). At the time of collapse, the core temperature should be 105 degrees F or higher; if cooling has been attempted prior to taking the temperature, mental status changes at the time when the temperature was highest and elevated muscle and liver enzymes are to be expected. Of course there is no pathognomonic sign at autopsy.
HYPOTHERMIA
Defined to be core body temperature below 95F. Below 31C / 86F, our enzymes don't work well. As a person dies of hypothermia, the skin blanches (vasoconstriction, why?), then reddens (loss of vasomotor control, with resultant rapid loss of heat.) The latter effect probably explains why many people who are freezing to death remove their clothes. Death probably results from brain and/or heart dysfunction.
|
* Dr. Overman, past medical examiner of Jackson County, shared the following anecdote:
| 
|
 "The Little Match Girl" Death by hypothermia / child exploitation |
Local hypothermia damages tissue by freezing of water, resulting displacement of ions, and vasoconstriction and loss of vasomotor control. Everyone is familiar with frostbite (which can progress to gangrene), and lesser degrees of cold injury. Note that fingers may be frostbitten but not appear red until they are re-perfused. In this type of injury (and many others), damage to the nerves can produce the troublesome, longstanding COMPLEX REGIONAL PAIN SYNDROME (formerly "causalgia").
![]() Gangrene
Gangrene
From frostbite
WebPath Photo
CHILBLAINS is a curious inflammatory purpura (the histology shows a microvasculitis) that appears as sore purple spots on parts of certain people's bodies after cold exposure. Mysterious but not dangerous. I suspect microthrombi are the actual cause.
* Nobody understands the coagulopathy of hypothermia. Thrombin gets activated, DIC occurs, platelets get activated -- lots of things happen. See J. Trauma 44: 846, 1998.
Future pathologists: Was the body alive or dead when it went into the snow? Easy call! Sking frostbitten in life is purple (why?), and under the microscope you'll see vacuolated epithelial cells, edematous dermis, and engorged capillaries (AJFMP 31(1): 18, 1992).
{07557} hypothermia
TORTURE
Inflicting severe pain as a means of coercion.
|
We'd all prefer not to hear or talk about this (most med schools never mention it: JAMA 276: 1676,
1996), but it's part of our world. The fact that these practices go on today
is testimony to human evil and
human (usually governmental)
ability to find justification for wicked practices. Alleged to be
government policy, typically used by one-party states for discouraging dissent,
in >80 countries in
the past ten years. What "counts" nowadays as torture is itself highly
politicized -- read today's headlines.
In combat situations with soldiers' lives depending on a prisoner talking, coercive interrogation (torture or the threat of torture) is and has always been a fact of life on all sides. This is especially true in a tactical situation. If the prisoner knows that the interrogators will discover the truth soon enough, the prisoner is likely to tell the truth, knowing that if he lies, he will be tortured for punishment. For me, this is far different from torture for political repression or to obtain confessions that might or might not actually be true. You might not agree. |
|
The accuracy of information obtained using torture has been discussed some in the medical literature since the September 11 terrorist attacks. A person under torture will do whatever they think they need to do to get it to stop. The "pop claim" is that under torture, the bad guy tells the truth because of an animal instinct to survive and/or because his cognition is impaired. One could only wish that a barbiturate infusion ("truth serum") worked better. Obviously we can't do good controlled studies, and life's taught me to be mistrustful of people's "impressions" especially when it comes to the behavior of people they do not like.
If torture does become legal and/or is widely practiced, they'll want a physician in attendance. Would you do it -- given that if you say "No", they're going to torture anyway and the victim is at greater risk of dying? That's a tough one for me. Regardless, the international standards for physicians (Declaration of Hamburg, Declaration of Tokyo, others) say you can't "abet" torture by your presence. See Lancet 373: 344, 2009; Lancet 375: 872, 2010.
* Democracies have historically limited the use of torture to anti-terrorism: Dan. Med. Bull. 37: 556, 1990, abstract 91160373; Br. Med. J. 308: 61, 1994; Am. J. Forens. Med. Path. 18: 321, 1997 -- Israeli security produces first known "shaken adult" fatality), or conditions in which there is a low-level race war (Lancet 344: 350, 1994); US forces, including health-care workers, in the rough interrogation of terrorists in Iraq and Afghanistan: Lancet 364: 725, 2004; Br. Med. J. 313: 1265, 1996. I've dealt with this in these notes for three decades; after 9/11, the question became much closer to home. Again, you'll need to decide whether this is morally acceptable and/or wise. In 2009, we were shocked by US Army psychiatrist Major Charles Burney's testimony that that torture was used to obtain FALSE confessions of a Saddam-Al Qaida link to justify the Iraq war to the American people. Watch this closely
* I would distinguish heinous torture (though you might not) from the rough-but-not-horribly-cruel, extra-legal police "street justice" that helps maintain public safety in communities where the official law doesn't work (as in high-crime areas of US cities). Ask me about this if you like; today's policeman is "damned if he does, damned if he doesn't", the winners are too-often the crybaby criminals and their lawyers, and the losers are decent people.
* The term "third degree" for harsh police questioning refers to medieval and early-modern protocols for torture on the rack (1st degree: shoulders, victim probably recovered; 2nd degree: elbows and knees, victim was crippled; 3rd degree: vertebral column, victim was paralyzed and died in hours or days).
| * Some countries use corporal punishment for criminal offenders. Delaware used whipping as an alternative to incarceration into the 1960's; the skin was almost never broken, and the purpose was to embarrass the perp and make it clear that punishment was being delivered without requiring time behind bars. Thankfully, we now sentence non-dangerous offenders to "community service" instead. |
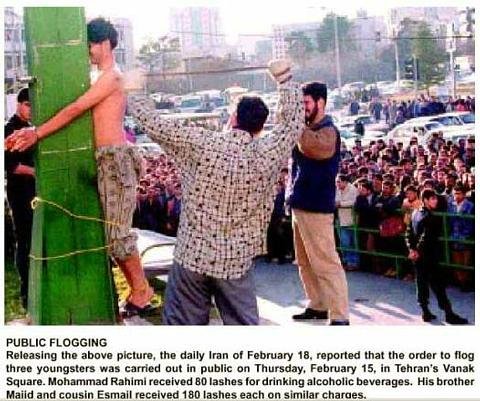 Flogged in Iran
Flogged in Iranfor drinking alcohol |
Of course, in our "enlightened" times, governments wish to avoid detection. Therefore, they prefer mental cruelty, sexual stuff (Lancet 336: 289, 1990; the methods are those that will not leave marks), near-asphyxiation, near-drowning, electricity from a magneto or charged object (field telephones and "stun weapons" are popular, delivering an agonizing but safe voltage), and application of electricity over a relatively large surface area (i.e., saline-soaked gauze pads between the skin and the jumper cables / magneto telephone; this is the world's most popular means of inflicting severe physical pain; review Am. J. For. Med. Path. 5: 333, 1984).
Low tech torture often involves beating with sandbags, which can rupture the guts without bruising the skin. When this leads to an agonizing death from peritonitis in a few days, there will be no external signs of torture, and the police will claim "heart attack". Chronic painful neuropathies are usual after other low-tech procedures ("Palestinian hanging", i.e., by the arms from behind in internal rotation, "falanga", i.e., whipping the soles of the feet), and beating and kicking the head is likely to begin chronic headache problems (For. Sci. Int. 108: 155, 2000).
Waterboarding has been famous through history as the one torture that breaks everybody -- even the Inquisition torture scene in "Melmoth the Wanderer" (1820) states that this is common knowledge. It seems to work by evoking a primal fear while producing little actual pain, and it leaves no marks and causes no physical damage. For more on this, read the newspapers.
* For lists of of practices in
Turkey ("Kurdish rebels"), and relative frequencies, see Am. J. Psych. 76: 76, 1994. Sikh radicals: Lancet 345: 225,
1995. Saddam's Iraq: Br. J. Psych. 172: 90, 1998.
Tibet J. Nerv. Ment. Dis. 186: 24, 1998.
Burma: Am. J. Pub. Health 86: 1561, 1996,
Br. Med. J. 312: 293, 1997. Bhutan: JAMA 280:
443, 1998.
The Maoist insurgency in Nepal (ceasefire April 2006)
tortured extensively: Lancet 358:
752, 2001.
Problems for doctors investigating claims of torture in Mexico: JAMA 289: 2135, 2003
("I'm sorry, we don't have a camera").
The Taliban was torture-happy: JAMA 280: 449, 1998.
Persecution of physicians by the Taliban: Lancet 355: 50, 2000.
Sierra Leone Lancet 353: 1365, 1999. Children and torture: Lancet 356: 2093, 2000.
Iran: J. Nerv. Ment. Dis. 185: 74, 1997.
Guatemala: J. Fam. Pract. 44: 209, 1997.
Mobutu's Zaire: Br. Med. J. 312: 293, 1996.
Survivors of the Vietnamese post-war "re-education camps": Arch. Gen. Psych.
66: 1221, 2009.
Zimbabwe's Mugabe tortures opposition politicians: Br. Med. J. 324: 317, 2002.
We're all heard the more recent tales, and in 2008, the British Medical Association
singled out the United States, Britain's ally in Afghanistan and Iraq,
for shocking even them by our systematic use of torture of terrorist suspects
(BMJ 336: 1458, 2008).
Syria's government-run hospitals turn in protesters who
have been shot so that they can be tortured: Lancet 378: 1606, 2011.
* Brain damage is common after some forms of torture,
and it is now being quantitated using visual evoked
potentials (Int. J. Leg. Med. 109: 114, 1996)
and imaging (Arch. Gen. Psych. 66: 1221, 2009).
Compared with government torture, the Italian Mafia
is surprisingly humane, even when executing its traitors:
Am. J. For. Med. Path. 19: 87, 1998.
The choice of suicide method after torture typically
mimics the torture method used (drowning, blunt force,
or stabbing): J. Tr. Stress 11: 113, 1998.
People who have been genuinely tortured usually have post-traumatic stress disorder (intrusive memories, "increased arousal", i.e., jumpiness) and particularly sleep disturbances. These seem to be fairly predictable in survivors (J. Nerv. Ment. Dis. 177: 147, 1989), and in fact having been tortured is the strongest predictor of future post-traumatic stress disorder (Br. J. Psych. 162: 55, 1993). Treating survivors: J. Nerv. Ment. Dis. 179: 4, 1991; JAMA 272: 357, 400, & 600, 1994; Br. J. Psych. 166: 705, 1995. After many years of practice, it's not clear that the well-known twelve-steppish mental health intensive rehabilitation of torture survivors does any good (J. Nerv. Ment. Dis. 198: 824, 2010). Commitment to a cause, a strong social support, and prior knowledge and preparedness seem to be helpful in preventing the most severe post-traumatic stress disorder, but the after-effects are still serious and long-term (Am. J. Psych. 15: 76, 1994). A group of psychiatrists examining US practices since 9/11 concludes that since humiliation, degradation, and helplessness without severe pain also seem to cause PTSD, they should also be illegal (Arch. Gen. Psych. 64: 277, 2007); as you'd expect, other commentators disagreed.
More than 100 countries now condone the use of torture, and a third to a half of victims claim that a physician was in attendance overseeing the torture (BMJ July 31, 2008). Other physicians have demonstrated real heroism in resisting these practices, and trying to control them (Iraq: JAMA 298: 494, 2007; Nepal and Rwanda Lancet 370: 698, 2007). Pathologists have risked their own lives to investigate claims, even in countries where "everything is okay now" (Nature 427: 664, 2004). Other physicians have cooperated (Saddam's doctors: JAMA 291: 1480, 2004). As with the other problems of the poor nations, the outlook is "guarded" or worse. Encouraging news (from the Danes) include (1) no claimants since the mid-1990's from Latin America, and (2) no reports of physician complicity.
Because of attempts to avoid detection, it may be difficult to determine whether a person seeking political asylum is simply making up a story. Presently, there are attempts being made to make this scientific, but it's still a real challenge. See For. Sci. Int. 76: 69 & 77, 1995; update from Denmark Am. J. For. Med. Path. 26: 125, 2005; from the USA J. Nerv. Ment. Dis. 199: 3, 2011. For now, if you are asked to assist with such a determination, I recommend:
IONIZING RADIATION
cosmic rays: Matter at relativistic velocities, from supernovas in distant galaxies, etc., etc. The particles they produce on colliding with our atmosphere are (along with terrestrial isotopes) the source of the natural background radiation.
curie: A unit of isotope that undergoes 3.7 x 1010 disintegrations per second.
gamma ray: A high-energy photon, capable of ionizing atoms and mutating your genes
half-life: How long it generally takes for half of the atoms in a sample of isotope to disintegrate
LET: "Linear energy transfer". A measure of the penetrating power of a form of radiation.
rad: A dose of energy resulting in absorption of 100 ergs per gram of target tissue. Abbreviated "r".
Gray (Gy): 100 rads. The LD50 for total-body ionizing radiation for a human is 3.5-4.0 Gy.
REM: "Roentgen equivalent for a man". A measure of the power to damage cells. Same as "RBE -- Relative biological effectiveness."
roentgen: How much radiation results in emission of one electrostatic unit of charge in 1 cc of air
x-ray: A human-made gamma ray.
* Target theory: Mathematical modelling for the statistical aspects of radiation injury and chemical carcinogenesis. "Single target theory" would have no minimum threshold for harm from radiation. This makes no sense biologically and doesn't fit with the empirical data, i.e., anybody offering this idea today is a crook.
"Big Robbins" describes the effects of ionizing radiation in much detail. You're already familiar with the generation of free radicals, which (whatever the details) is how gamma rays do their harm to living tissue. Here's what's worth learning now:
The most radiosensitive normal tissues are lymphoid organs, bone marrow, and germ cells. Not surprisingly, the most radiosensitive tumors are lymphomas, leukemias, and seminoma/dysgerminoma.
Cells that normally divide a lot (i.e., epidermis and its adnexa, GI mucosa, bronchi) are more vulnerable to radiation than most other organs. Germ cells and lymphocytes also carry the instruction: "If you're hurt, then die, don't divide." (Why might that be?) Bone, muscle, cartilage, and nerve are highly radioresistant. Except as noted above, the susceptibility of a cancer to radiation has little to do with the susceptibility of its parent cell.
During the weeks after therapeutic radiation, there's considerable proliferation of blood vessels; you'll be able to see this yourself. Possible mediators: Am. J. Path. 171: 338, 2007.
Under the microscope, pathologists recognize two features of radiated tissue.
1. The vessels exhibit exaggerated hyaline sclerosis; much like the arterioles in diabetes and hypertension, but more extensive and worse. This narrowing of vessels continues to get worse for the rest of the patient's life. (In the acute phase, look also for obvious injury to the endothelium; at high doses, look for fibrinoid necrosis of vessels.) Review J. Laryngol. Otol. 111: 988, 1997.
2. Scattered cells often exhibit large, hyperchromatic nuclei that one could mistake for cancer cells. Probably what's happening is that the radiated cells can duplicate their DNA in preparation for division, but cannot divide.
* Today's procedure to find sentinel nodes involves injecting the tumor site with radioisotope, finding the node with the Geiger counter, and sending it to the pathologist. Dealing with radioactive specimens: Am. J. Clin. Path. 134: 299, 2010.
|
RADIATION SICKNESS
While it is commonplace to dose a part of the body with 4000-5000 rads to kills cancer cells, a total-body dose of radiation will have the following untoward effects. |  Russian sub K-19, mostly-true story |
You will calculate the rads/Gys received by the time it takes from exposure to the onset of vomiting, the rate of lymphocyte depletion on serial CBC's, and the presence of chromosomal aberrations.
200- 500 rads
HEMATOPOIETIC SYNDROME. Early nausea and vomiting on the first day. Afterwards, blood cells disappear from the body (lymphocytes first, since they are the most vulnerable; afterwards, short-lived neutrophils and platelets; ultimately, survivors become anemic.) Victims receiving 200 rads will probably survive; those receiving 500 rads will probably die.
500-1000 rads
GASTROINTESTINAL SYNDROME. Severe nausea and vomiting occur within a few hours, and are only the most prominent symptom in a body in which many cells have died in many places. Most victims will die in a few days.
>5000 rads
CEREBRAL SYNDROME. Brain necrosis and edema will produce drowsiness, coma, and death in an hour or two.
In survivors of Hiroshima and Nagasaki, the following additional health effects were noted:
|
|

|
In survivors of Chernobyl, the following additional health effects were noted:
American service personnel exposed during the atomic tests after WWII do not seem to have any increased total cancer risk or total mortality (Occ. Env. Med. 60: 165, 2003).
* One often-discussed idea for a petty tyrant's nuclear weapon ("dirty bomb") is a conventional bomb packed with radioactive waste from a nuclear power plant.
* Goiania is a town in Brazil where some lowlifes stole Cs137 from an abandoned radiation therapy unit (!); the glowing particles ended up being distributed as "carnival glitter" (!!). The result was a lot of radiation sickness and some deaths (Mut. Res. 373: 207, 1997).
You'll learn in the clinic about the deleterious effects of therapeutic radiation. Pulmonary fibrosis has long been well-known. Many people still do not appreciate that therapeutic radiation to the brain, while it may help control cancer, will often produce appalling brain damage (Cancer 63: 1962, 1989).
The worst scandal in American forensic science was the case of Joyce Gilchrist, Oklahoma's forensic chemist, who on the evidence simply fabricated whatever evidence police and prosecutors wanted. Read about her here, here, here, here, and many more. West Virginia's Fred Zain left a similar record of falsified evidence in the 1980's.
FUTURE PATHOLOGISTS: THE NEGATIVE AUTOPSY ("OBSCURE AUTOPSY")
{25532} x-ray burn
 | Mass grave at Auschwitz |
-- Brihadaranyaka Upanishad (Hindu scripture)
--Anakin Skywalker
Do you love your Creator? Love your fellow-beings first.
-- Muhammad
Lord, make me an instrument of your peace.
Where there is hatred, let me sow love,
where there is injury, pardon,
where there is discord, union,
where there is despair, hope,
where there is doubt, faith,
where there is darkness, light,
where there is sadness, joy.
O divine master, grant that I may not seek so much
to be consoled as to console,
to be understood as to understand,
to be loved as to love.
For it is in giving that we receive,
it is in pardoning that we are pardoned,
and it is in dying that we are born to eternal life.
-- Attributed to "Francis of Assisi" (John Bernardone) c. 1230
-- Albert Einstein (Christian Century, 8/28/1929)
--Martin Buber
|
The ballot is stronger than the bullet. --Abraham Lincoln 5/19/1855 Who overcomes by force has overcome but half his foe. --John Milton, "Paradise Lost" I am proud of the fact that I never invented weapons to kill. --Thomas A. Edison, NYT 6/8/1915
|

|
 |
I think that people want peace so much that one of these days governments had better get out of the
way and let them have it.
-- Dwight D. Eisenhower, 8/31/1959 |
|
If any question why we died, Tell them, "Because our fathers lied".
Formerly England's most popular pro-war poet,
|
|
Violence usually begins with invasion of someone's personal space, respect, or dignity. Everyone feels entitled to these things, whether or not everyone else agrees.
Despite the attention given to RANDOM VIOLENCE, especially in our slums, in recent decades, most homicides are still committed by SOMEONE THE VICTIM KNOWS. The larger story of any homicide or suicide seldom shows the finer side of humankind. Your lecturer is no expert on security or crime prevention, but he's had considerable reading and professional experience relating to homicides.
The following suggestions will not make you immune to becoming a homicide victim, but will greatly reduce your risk of dying at the hand of someone you know:
|
1. Don't bully anyone, physically or verbally. 2. Don't ridicule anyone. (This is a really important survival tip.) 3. Don't try to take another person's wife or girlfriend. 4. Don't crowd or speak rudely to a person who is obviously upset, even if he or she is threatening you or someone else. 5. When a relationship breaks up, be tactful and kind to the person to whom you were important. 6. Don't deal drugs. 7. Don't do sexual things for money or drugs. 8. Men: Don't carry a weapon. (This applies in the vast majority of circumstances. There are exceptions.) 9. Women: Don't be a sexual tease. |
Val Kilmer's Hamlet |
10. Gay men: Don't do sexual things with men you don't know well, or with jealous (i.e., nutty, insecure) men. Don't ask out men you don't know well. (Homicides: AJFMP 17: 350, 1997).
11. Don't become emotionally close with not-perfectly-controlled schizophrenics, or imagine that you can help them with "love".
12. Married women: Move out of the house and stay away from your bad-tempered husband BEFORE you tell him you are going to divorce him and take everything that he has.
13. Women: Don't be pregnant by a man who does not want to be your child's father (Am. J. Pub. Health 95: 471, 2005 gives the numbers -- the conclusion seems to follow though it's not stated in so many words; also Ob. Gyn. 115: 1181, 2010.)

Huck Finn |
14. Children and teens: If the adults with whom you must live are abusive, pretend you love them anyway until you are able to escape safely. (The murders of non-gang teens, especially girls age 11-14, are typically by a parent "following an argument" -- Arch. Ped. Adol. Med. 157: 355, 2003). Revenge (or forgiveness) can wait -- survive for now, and you'll get your chance. Of course, this also applies in the much-described "intimate partner violence" situation -- today, most victims escape before being murdered thanks to the attention that the syndrome is (rightly) receiving. Nowadays in the US, only about 35% of murders of women are known to be intimate-partner violence (it was once probably much higher); around 6% for men. Worldwide, things are still less encouraging (Lancet 382: 859, 2013) -- for intimate partner homicides, there are six man-kills-woman for every one woman-kills-man. In murder by a present or past intimate partner, the woman's friends and children are likely to be killed as well. |
There are social networks of violent people ("the knife and gun club") -- people who are socially networked with people with a history of violence are much more likely to be murdered (the African-American experience Am. J. Pub. Health 104: 143, 2014). Sociobiology in action: Living with a step-parent is the most powerful risk factor for child abuse yet identified. See Science 261: 987, 1993. A child in Canada is sixty times more likely to be murdered by a step-parent than by a parent: Sci. Am. 273(4): 174, Oct. 1995. Readers will not be surprised that in the US, infanticide is far more common if Mom is less than 17: NEJM 339: 1211, 1998. The mentally ill are much more likely that healthier folks to be murdered: BMJ 346: f557, 2013 (substance abusers ~9x, personality disorder without substance abuse ~3x, schizophrenia without substance abuse ~2x, etc.; this is not surprising.)
* Child-kills-parent: rare. Usually Dad is murdered, usually for being a control freak.
* In the townships of "the new South Africa", a child is almost as likely to be killed in cold blood (often shot to death, something that almost never happens in the U.S.) as he/she is to die in an accident (Am. J. For. Med. Path. 24: 141, 2003).
NOTE: Alcohol is a factor in a majority of homicides. Certain men, under the influence of alcohol, are prone to fire their handguns at other people for no reason. Even when there is some motive, a majority of murderers have alcohol on board at the time of the crime, and a majority of victims have alcohol on board.
NOTE: When there is a motive for murder, other than disputes among drug-culture types, sex is
almost always involved, and usually somebody has insulted
the murderer's pride in this particular
area. The most classic of all non-underworld, non-underclass homicides is the man who kills the
woman who left him.
* NOTE: There are around 20,000 murders yearly in the US (J. For. Sci. 42: 279, 1997).
The one situation in which no doubts that the death penalty is a deterrent is to prevent the
murder of a witness -- if someone has already committed a heinous crime, they have no reason not to
kill the principal witness against them unless the threat of the death penalty hangs over them.
"If a man kills one person, he's a criminal. If a man kills 100,000 people, he's a hero."
Whether the violence is individual or institutionalized, violent people will surprise you by their
selective delicacy of conscience. They may be crusaders for good causes and pillars of the local
place of worship, exhibit extreme tenderness toward children, the sick, the elderly, and so forth.
Hitler and Ted Bundy embraced vegetarianism,
because they professed to abhor harming innocent creatures. Hitler was opposed
to using animals for medical research.
Lancet reports that since 1973, 139 people on American death rows have been exonerated
after an average of 9.8 years in prison (Lancet 375: 1516, 2010). This doesn't surprise me.
* Easy, wrong answers:
If "violence in the movies and on TV" is a major factor in our epidermic of violence
(as suggested in JAMA 267: 3059, 1994), why is the murder rate 10 x lower in Canada, where they
watch the same shoot-'em-ups?
See Lancet 365: 702, 2005 (if there's a causal link, it's weak and hard to study);
J. Ped. 154: 759, 2009 -- concludes violence in the media does not
produce increased aggression. And if handguns are the problem, why is the
murder rate similar in non-inner-city Canada (where murderers use knives and bludgeons) and non-inner-city areas our own states
that adjoin Canada (where gun ownership is much higher, and the
murderers use guns; see Am. J. Epidem. 134: 1245, 1991)? More on international comparisons:
JAMA 263: 3292, 1990. In some US elementary and high schools,
most of the students are armed with guns simply for self-protection,
yet there
are surprisingly few shootings, and the kids are far safer
in school then outside. Although there is much less legal gun
ownership in Sweden, there are still plenty of mass-shootings:
AJFMP 19: 34, 1998.
Murder rates per 100000 people per year worldwide: South Africa 75.3 (Am. J. For. Med. Path. 24: 141, 2003),
Philippines 38,
Lesotho 36, Jamaica 18, US 8, France 4, Britain 1.3, Ireland 0.5. Obviously there's something more
than "guns cause murders". A Jamaican pathologist's perspective: Br. Med. J.
335: 1097, 2007. More easy explanations that aren't true...
The familiar right-wing claim that more people have died violently
since the 1859 publication of "The Origin of Species",
and the familiar left-wing claim that "science leads to a devaluing
of human life", both
ignore the fact that the world is more densely populated today
thanks to science (public health, fertilizer); nevertheless,
Tamurlane probably killed
as many people as Hitler did in his own era. The familiar right-wing
claim that child abuse is a new phenomenon caused in particular
by the decline in "family values"
ignores the fact that physicians
simply denied, ignored, or covered it up during the "good old days" before the
1960's.
Reading about how we "discovered" why some babies have multiple
fractures of different ages is chilling. Society calls for
radical changes in the wake of
shooting sprees (by loonies whose neighbors knew something was
badly wrong, by high-school kids who were teased and ridiculed for
years by their "well-adjusted" peers, and so forth). But
at the same time, society goes gah-gah when
honest scientists try to look at the impact of genes or brain chemistry
on bad behavior, or when people talk about putting obviously dangerous,
mentally-ill people in long-term institutional care.
On average, 20% of welfare schizophrenics will commit a violent act and/or
threaten someone with a lethal weapon during a six-month period
(Arch. Gen. Psych. 63: 490, 2006;
Am. J. Psych. 163: 1404, 2006), and for those who are rampaging
around and having delusions of persecution, the risk is much higher;
all that American society is able to do at present is either think of ways to keep
particular individuals in jail, or leverage their welfare checks, which
(2006) has the lawyers in an uproar.
Diagnosed bipolars are also more than twice as likely as normal folks to be violent (Arch. Gen. Psych. 67: 931, 2010).
Again, there are no easy answers.
* To compound the mystery... During the early 1990's, the rates for murder,
assault, robbery, and burglary all dropped precipitously in the US.
The causes remain obscure (Sci. Am. 290(2): 82, Feb. 2004).
The epidemic of murder among black and hispanic men ages 14-24
peaked around 1991 (5x above the usual
norms, 1 in 20 ended
up being murdered by a peer in some communities) and is dropping, perhaps because
crack use is being replaced by marijuana use, and marijuana dealers are a non-violent
bunch (uh...?)
Booming economy (timing's off)?
Roe v. Wade causing fewer unwanted neglected children (timing's off)?
More cops (NYC experience)?
Concealed-carry (maybe)? More prisons with the bad people off the streets (uh, this isn't the "politically
correct" answer, but it's the one I find easiest to believe)?
Crime prevention as a public health measure is reviewed in Britain's Lancet 358: 1717, 2001;
it holds America's ugliest statistics up for examination, and points what has worked
and what hasn't; its explanation for the drop in our murder rate is the policy by the
police to focus their attention ("by the book" or not)
on the really bad people and the really bad places. The statistics
(a 1% increase in prison population reduces murder by 1% and violent crime by about 2%)
seem to confirm the common-sense idea that keeping bad people off the streets
until middle-age settles them down
is also helpful. Simply increasing the numbers of officers is supposedly less helpful,
and the "zero-tolerance" nonsense (i.e., busting kids for having nailclippers
or an aspirin) does no good.
* The sleepwalking defense after a violent crime: Nobody knows. See
Am. J. Psych. 161: 1149, 2004.
* You heard it here first. Today's polygraph testing is
considered by some to be reasonably useful especially for criminal
investigations (JAMA 256: 1172, 1986 -- also deplores using it as the
sole basis for screening your employees for crooks to fire), or as
a parlor trick, mere salesmanship-and-subscience (NEJM
327: 122, 1992, Lancet 360: 1261, 2002,
The fact that a bunch of Castro's people all beat
the polygraph to go to work for the CIA some years back,
tells something.) It is impossible to do really
controlled studies, but my impression after 20 years hanging
around criminal justice is that a polygraph operator with
integrity and skill can usually give an accurate reading,
and that not all operators possess skill-plus-integrity.
The Japanese experimented with brain wave patterns
that indicate whether a suspect recognizes, or does not recognize, a crime scene. Sounds
interesting. For. Sci. Int. 51: 95, 1991. Brain mapping for deception and truth telling:
Radiology 238: 679, 2006.
More generally, your lecturer has fair
confidence
in the criminal justice system's ability to discriminate guilt from innocence, usually,
with the unique
exception of men falsely accused of sex crimes. This is what the inmates themselves told me in the
1980's, and my own experiences and reading bear this out. In today's political climate, an innocent
man must often plea-bargain and even serve prison time (Science 256: 301, 1992; KC Star March
13, 1993; remember also Potiphar's wife Genesis 39:7-20). This has
now become a public
scandal, as happened with the "false memories"
fiasco of the early 1990's and the ultra-bizarre, no-physical-evidence
child-molestation witch-hunts ("Believe the children!")
of the past 40 years.
In the
meantime, men, you must "love defensively", and you shouldn't even talk at all to a woman unless
you know she isn't crazy. Of course, women have always known not to talk
to a man until she knows he isn't crazy, because there is still plenty
of real violence and abuse.
* Punch-and-Judy have been
considered funny, but domestic violence isn't.
Wife-beating (and girlfriend-beating, and of course child abuse) continues epidemic despite the fact that it's
receiving much more attention lately (as it should). About 1.5 million women in the US
experience "intimate partner violence" each year (JAMA 288: 589, 2002;
this is still too many though it may be fewer than you've been told).
Around 10% of emergency room visits by adult
women result from their getting beaten in an ongoing man-beating-woman situation (JAMA 1995;
discusses the error in Am. J. Psych. 151: 630, 1994 by militant feminists who claimed the number
was 35%). He is often an alcoholic bully or junkie with scrambled brains, but the stereotype doesn't
always hold. Psychiatrists talk about insecurity as the basis for the habitual wife-bearer's part (gee whiz),
and so forth. A small minority are sociopaths, i.e., charming, personable men who are incapable of
acting from moral principles. While they were dating, she liked his aggressive, assertive style. Now she's
sorry, but where would she go? Plus, she likes it when he apologizes and makes up each time (even
after she has him arrested). If she is a nagger, things become even worse. When a man kills a woman, it's likely that this stuff has been going on
beforehand. Both partners usually have lousy overall living skills, though sometimes the woman is
well-educated and/or hard-working and just has poor people-skills.
Because of politics, if she beats him, or both
beat each other, or if he even grabs her arms to keep her from hitting or
scratching him, the system still focuses on him as the problem.
With the focus on
"keeping the family together to keep Mom off welfare", the problem will get worse. Some of these
people may be educable, for their sake and for the kids'. In the meantime, your first concern as a
physician is the physical safety of the woman and children.
Exactly what to do to help in the long-term is much tougher to know;
getting women to shelters and to advocacy seems to help, nobody really seems to have
anything that helps the men be better husbands / boyfriends,
and there are risks of causing reprisals (JAMA 289: 589 & 601, 2003).
* Whether it's abuse of a child or a romantic partner, the behaviors of the
abuser are pretty much stereotyped, and you will come to recognize the
constellation. The common denominator, of course, is that THE ABUSER FEELS ENTITLED TO
LOVE, and has such poor living skills that he or she cannot get it
any other way. Public discussions usually ignore this obvious fact, but
understanding it may help you, the physician, help people make sense out of the
vicious cycle.
The crew at Galveston has finally gotten
up evidence to show that, yes, beating a pregnant woman can give her preterm labor and
chorioamnionitis (Am. J. Ob. Gyn. 170: 1760, 1994). 
* NOTE: Criminality has no easy explanation. The classic parents of a criminal (an
alcoholic bully
father, a hysterical pill-popping mother) are folks whom you'll meet soon enough, but many
criminals come from "nice homes", and most brothers of hardened career criminals have no criminal
records themselves. For decades, the social psychologists
have insisted that "violent criminals
suffer from low self-esteem", and based "treatments" on this ideology.
A review team found that there was never been any empirical evidence that this is true.
Having known a few, I tend to agree with the team that they are mostly big-ego
types who have decided they are special, above the law (Sci. Am. 284(4):
96, 2001).
Other "enlightened" explanations for criminality just don't fit the facts either: Poverty isn't the
explanation, since self-reports of misbehavior correlate very little with class. Most poor folk are
decent, law-abiding people who hate the criminals among whom they must live. Despite much
effort, nobody's been able to demonstrate that police and courts treat blacks and whites differently if
they've done the same bad things. Injustice isn't the explanation, since police, victims, and criminals
all agree about what's right and wrong and what should be done with wrongdoers. A few traits of
career criminals are well-known: (1) they socialized poorly as kids; (2) they were poorly supervised
by their parents; (3) they are sensation-seekers and continually seek new excitement; (4) by any
reasonable definition, they are racists; (5) they drink alcohol; (6) they have never been seriously
interested in serious religion; (7) they suffer less from a bad conscience than do the rest of us. I
would have added (8) they are demanding of everyone except themselves; career criminals are the
worst crybabies. Most criminals learn early to cite past wrongs (personal,
ancestral) to gain sympathy and special privileges.
There's a review in Nature 368, 111, 1994. There's a adoption study that
concluded that childhood misbehavior was mostly caused
by the environment, but found that your number
of adult convictions correlated better with convictions of your biological parents rather than your
adoptive parents (!!; Lancet 345: 466, 1995; has a list of candidate genes).
Studying behavioral genetics has been a problem historically.
When Brunner's disease (mutant monoamine oxidase A producing mild mental retardation
and outbursts of senseless violence) was described (Science 262:
578, 1993), the discovers were smeared by media for political
incorrectness. This seems to have stopped.
A man always finds it hard to realize that he may have finally
lost a woman's love, however badly he may have treated
her.
"Sherlock Holmes", "The Musgrave Ritual"

Punch and Judy
Suicide is a permanent solution to a temporary problem.
--Phil Donahue
Here's a list of principal reasons people take their own lives. This pathologist's impression is that this is approximately the sequence from most-common toward least-common. It is not exclusive, but covers the large majority of cases. This list is among the greatest of all monuments to human stupidity and cruelty, typically by those surrounding the ultimate victim (there are exceptions).
|
1. Failed relationship... (any age, either sex) 2. Organic mood disorders... (young and middle-aged adults) 3. Financial disaster... (adult men -- the Swedish experience during the recession Am. J. Pub. Health 103: 1031, 2013). The most malignant cause is problem gambling. 4. Chronic poor health... (teens and adults, either sex; suicide in older folks is very often triggered by impending nursing home placement) 5. Abuse (physical or verbal) by a parent... (older children, teens)
6. Fear of being a homosexual... (teens and up, mostly men; see Am. J. Pub. Health 92: 1338, 2002; nowadays it's most likely to happen if the person has been ridiculed / bullied by parents or at school or work: Am. J. Pub. Health 103: 70, 2013) 7. Bad body image... (teens, younger adults) 8. Schizophrenia... (teens and adults, either sex) 9. Being arrested (trigger for suicide in high-achievers in difficult situations) |  |
School failure is probably less common than any of these causes of suicide. Athletic failure is also less common.
* Suicide in veterans of the Iraq and Afghanistan wars is common but -- and I was surprised too -- seemingly unrelated to what had happened to the veteran during the war. See JAMA 310: 496, 2013. Suicide in the army personnel on active duty parallels civilian life -- job stress, failed relationships (Am. J. Pub. Health 102-S1: S-40, 2012).
* The truly hard-core will enjoy studies that show different genes are methylated in the hippocampus in suicide-completers and controls: Am. J. Psych. 170: 511, 2013.
* The surgeons, not noted for being tender-hearted, tell it straight -- during residency, you WILL experience depression and suicidal thoughts. Surviving: Am. J. Surg. 205: 141, 2013.
NOTE: Alcohol is a contributing factor to the crisis that precipitates the suicide in at least 1/3 of cases, probably more.
NOTE: Illegal drug use will exacerbate any of the above problems.
NOTE: The large majority of suicides have had no contact with mental health services, even though they are widely available and the easier and more convenient they are to access, the lower the suicide rate (Lancet 379: 981, 2012).
NOTE: In the developed world, the suicide rate among young men (ages 15-34) has been dropping dramatically since about 1993 (BMJ 336: 515 & 800, 2008; others). Your lecturer believes that this is because of the internet, where people can find friends, support, opportunities, and accurate information. The deadliest warning sign -- withdrawal from friends -- keeps the support system from functioning unless the friends are VERY alert. The availability of good antidepressant medications, and the hope they offer, probably contributes as well.
Reactive depression usually results from being dumped or being trapped; both are more depressing than the death of a loved one (Arch. Gen. Psych. 60: 789, 2003). In "conservative traditional societies", it is commonplace for a teenaged girl to commit suicide after being forcibly "married" to a man she hates (Am. J. For. Med. Path. 24: 214, 2003.)
You will accomplish nothing with the suicidal patient by simply listening sympathetically. Help them solve their current life problems, and learn problem-solving skills. Help them monitor their thoughts -- your feelings about your situation are perhaps valid, but you are not helpless, you do not need to be unlovable, you can tolerate distress even though it goes deep and is physical. Look at what you have done RIGHT so far, the progress you've made, and can you think of any advantages of being alive over being dead.

|
You can find something better than death everywhere.
|
| * Shakespeare's Hamlet in the soliloquy is asking "Is life worth living?" He calls death "the undiscovered country" from which "no traveler returns" despite (according to Shakespeare's sources) having recently talked with a ghost. This is probably intentional. Despite the trappings of supernaturalist religion, Hamlet could be any post-Age-of-Faith person considering suicide. |
|
|
NOTE: AMONG PHYSICALLY-HEALTHY YOUNG PEOPLE WHO ATTEMPTED SUICIDE, FAILED, AND GOT APPROPRIATE FOLLOW-UP CARE, 99% ARE PLEASED, ONE YEAR LATER, THAT THEY FAILED. In the vast majority of cases, the situations that precipitate suicide of a person in decent physical health are temporary. For a more recent, pretty-much equally optimistic study from Vanderbilt, see J. Traum. 33: 457, 1992; in addition to the familiar truisms, intervening in crazy family situations seems to be critical. |  |
![]() Crime Scene
Crime Scene
Online fantasy site
"Current investigations"
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about forensic pathology to consult these standard textbooks.
More good reading: My favorites in training were...
Spitz, W.U., and Fisher, R.S., "Medicolegal Investigation of Death", ed. 2, Springfield: Thomas, 1980. Do not read chapter 19.
DiMaio, D.J., and DiMaio, V.J.M., "Forensic Pathology", New York: Elsevier, 1989.
"American Journal of Forensic Medicine and Pathology" (AJFMP). Great for study-breaks; the KCUMB library's subscription begins in 1993.
In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!

| New visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request
| If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |
Teaching Pathology
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 |
Taser Video 83.4 MB 7:26 min |
 |
Click here to
see the author prove you can have fun skydiving without being world-class. Click here to see the author's friend, Dr. Ken Savage, do it right. |


 Forensic Medicine for Medical Students
Forensic Medicine for Medical Students








 * All about the "war on drugs": NEJM 330: 357, 1994; JAMA 273: 1143, 1995,
Lancet 357: 971, 2001; "a quagmire for our times J. Pub. Health Policy 23: 286, 2002;
BMJ 341: c3660 & c4610, 2010
Historians regard the draconian anti-heroin laws of the past
as a disaster for good citizens and addicts alike (J. Soc. Hist. 44:
71, 2010).
It is one of the mainstays of "politics as usual".
Talking about this subject is now considered appropriate for the classroom.
The war on drugs
directly consumes about $17 billion of our tax dollars per year. There are around 3.5-4 million
hard-core addicts (cocaine, crack, heroin), mostly underclass, who are
doing most of the crime (robbery, shoplifting, low-level dealing,
also child neglect and abuse.)
Nobody likes people being addicted to drugs like cocaine and heroin. But
despite the rhetoric, it is obvious that vested interests
are in control of drug policy.
Addiction treatment on demand
remains unavailable for most people (Am. J. Psych. 151: 631, 1994; Forens. Sci. Int. 62: 129,
1993; Am. J. Pub. Health 89:
657, 1999).
The unavailability of treatment is, of course, the result of politics. (Nancy Reagan's
"Just Say No!" campaign, the Republican-Right response to conservative suburbanites
who wanted the government to focus on preventing their children from
smoking marijuana, ended the Nixon-Carter policy of quietly providing
detoxification. Conversely, communities that profit massively from the drug
trade strongly oppose detoxification -- their
left-wing rhetoric is "curious".)
Thankfully, cheap detoxification is becoming
more available, but for decades, an addict would have to wait
months; this satisfies me that neither the "liberal" nor the
"conservative" politicians really wanted criminals/addicts off the streets.
(You'll hear the current strategy of interdiction compared to
the game "whack-a-mole".
Notice that neither "liberal" nor "conservative" politicians
ever talk about military action against the cocaine and heroin
lords. Is this because they both benefit from
the status quo? Or is it because they realize that this
wouldn't work?)
Drug addiction is notorious for relapsing, and no one expects
that methadone maintenance patients will really remain free of
street drugs, only that the maintenance will diminish their illegal
activities (JAMA 281: 1000, 1999).
Drug-related crime has turned our inner cities into war zones
(there were around 1500 drive-by shootings in 1995 in Los Angeles alone),
young children are brought into criminal lifestyles by drug dealers
since they will be punished less severely when caught,
and drug-related crime
is the #1 or #2 concern of Americans in the surveys lately
(after the health-care mess of course).
Pediatrics 93: 1050 & 1065, 1994
showcases the disastrous effects on black males ages 9-15; this is one you oughta read, though I
don't know whether the "multilevel strategies" the left-wing authors propose will solve the problem
while the "war on drugs" continues and there's easy money to be made by those who are not "future-oriented".
Drug availability
is undiminished (because it is illegal, a high school kid has a much
easier time getting marijuana than alcohol),
and the number of deaths from drug overdose (not to
mention the associated crime and that retroviral disease that is still increasing among IV drug
abusers) continues to increase. At least we are putting away more drug dealers, who now occupy a
third of our penitentiary spaces (additional $$ beyond the $17 billion/year). Parents: If you don't
take a personal, friendly interest in your kids and their happiness, then the local drug dealer
probably will. And if
you have offered your kids nothing credible to feel part-of, then the local drug culture
probably will. The case for
continued prohibition of the recreational drugs is persuasive for many people (who generally assume
that decriminalization / legalization would increase drug use, which you might reasonably doubt).
But their arguments could be applied equally well to alcohol and tobacco (Nature 374: 391, 1995) -- but you knew that.
* All about the "war on drugs": NEJM 330: 357, 1994; JAMA 273: 1143, 1995,
Lancet 357: 971, 2001; "a quagmire for our times J. Pub. Health Policy 23: 286, 2002;
BMJ 341: c3660 & c4610, 2010
Historians regard the draconian anti-heroin laws of the past
as a disaster for good citizens and addicts alike (J. Soc. Hist. 44:
71, 2010).
It is one of the mainstays of "politics as usual".
Talking about this subject is now considered appropriate for the classroom.
The war on drugs
directly consumes about $17 billion of our tax dollars per year. There are around 3.5-4 million
hard-core addicts (cocaine, crack, heroin), mostly underclass, who are
doing most of the crime (robbery, shoplifting, low-level dealing,
also child neglect and abuse.)
Nobody likes people being addicted to drugs like cocaine and heroin. But
despite the rhetoric, it is obvious that vested interests
are in control of drug policy.
Addiction treatment on demand
remains unavailable for most people (Am. J. Psych. 151: 631, 1994; Forens. Sci. Int. 62: 129,
1993; Am. J. Pub. Health 89:
657, 1999).
The unavailability of treatment is, of course, the result of politics. (Nancy Reagan's
"Just Say No!" campaign, the Republican-Right response to conservative suburbanites
who wanted the government to focus on preventing their children from
smoking marijuana, ended the Nixon-Carter policy of quietly providing
detoxification. Conversely, communities that profit massively from the drug
trade strongly oppose detoxification -- their
left-wing rhetoric is "curious".)
Thankfully, cheap detoxification is becoming
more available, but for decades, an addict would have to wait
months; this satisfies me that neither the "liberal" nor the
"conservative" politicians really wanted criminals/addicts off the streets.
(You'll hear the current strategy of interdiction compared to
the game "whack-a-mole".
Notice that neither "liberal" nor "conservative" politicians
ever talk about military action against the cocaine and heroin
lords. Is this because they both benefit from
the status quo? Or is it because they realize that this
wouldn't work?)
Drug addiction is notorious for relapsing, and no one expects
that methadone maintenance patients will really remain free of
street drugs, only that the maintenance will diminish their illegal
activities (JAMA 281: 1000, 1999).
Drug-related crime has turned our inner cities into war zones
(there were around 1500 drive-by shootings in 1995 in Los Angeles alone),
young children are brought into criminal lifestyles by drug dealers
since they will be punished less severely when caught,
and drug-related crime
is the #1 or #2 concern of Americans in the surveys lately
(after the health-care mess of course).
Pediatrics 93: 1050 & 1065, 1994
showcases the disastrous effects on black males ages 9-15; this is one you oughta read, though I
don't know whether the "multilevel strategies" the left-wing authors propose will solve the problem
while the "war on drugs" continues and there's easy money to be made by those who are not "future-oriented".
Drug availability
is undiminished (because it is illegal, a high school kid has a much
easier time getting marijuana than alcohol),
and the number of deaths from drug overdose (not to
mention the associated crime and that retroviral disease that is still increasing among IV drug
abusers) continues to increase. At least we are putting away more drug dealers, who now occupy a
third of our penitentiary spaces (additional $$ beyond the $17 billion/year). Parents: If you don't
take a personal, friendly interest in your kids and their happiness, then the local drug dealer
probably will. And if
you have offered your kids nothing credible to feel part-of, then the local drug culture
probably will. The case for
continued prohibition of the recreational drugs is persuasive for many people (who generally assume
that decriminalization / legalization would increase drug use, which you might reasonably doubt).
But their arguments could be applied equally well to alcohol and tobacco (Nature 374: 391, 1995) -- but you knew that.



 Organophosphate poisoning
Organophosphate poisoning Rural physician
Rural physician
 Hogarth's "Gin Lane"
Hogarth's "Gin Lane"