Presentation: Pregnancy
Title: Mother and Child
Date & Time: Monday, April 12, 2010 at 10 AM
Lecturer: Dr. Garcia and Team
QUIZBANK: "Fetus and Pregnancy"
{47859} pregnant
{08434} normal pregnant uterus, gross
{09780} normal pregnant uterus; baby below match-stick
{24666} normal placenta
{21104} normal pregnancy
{38995} normal pregnancy
{08928} normal placental villi in ectopic pregnancy
{08930} normal placental villi in ectopic pregnancy
{11024} placental infarct, gross; these are common and usually harmless
{49415} hydrops fetalis
{49416} fetal death, cord around neck
EXAMINING THE PLACENTA (stil good: Am. Fam. Phys. 57(5), March 1998)
Here's what to look for:
Thick placenta: Diabetes? Hydrops fetalis? Infection? All these should be known
to you already.
Big blood clot? Suspect that there was an abruption!
A few cotyledons fibrotic? Old infarcts. A few cotyledons overly red? New infarcts.
Infarcts happen and unless they are involve more than 5% of the surface
(typically much more), nothing to worry about.
Pale? Is the baby anemic? Is Mom bleeding out?
Soft? Infection?
Fleshy, dark red blob? CHORANGIOMA (CHORIOANGIOMA). A benign hemangioma, of no consequence
unless it is huge, in which case it acts as a shunt, consumes the baby's platelets,
and can cause congestive heart failure.
An accessory lobe, separated from the main placenta by vasculature,
is called a SUCCENTURIATE LOBE and the membranes are often
attached. If by misfortune this overlies the cervix, it's likely there'll be bleeding.
A BILOBATE placenta, with equal-sized lobes, carries the same risk.
CIRCUMVALLATE PLACENTA: The basal plate (mom's side) is quite a bit bigger than the chorionic
plate (baby's side); this will appear as a ring around the edge on the fetal surface.
This can cause various problems as you'd expect, since the baby's wrapped up inside.
A CIRCUMMARGINATE PLACENTA is a forme fruste that's not so worrisome.
AMNION NODOSUM is vernix caseosa embedded in the amnion. Usually there's
oligohydramnios. It should not be confused (though some do) with the
harmless squamous metaplasia you can see here especially near the insertion of the cord.
Any amnionic bands?
Green? Meconium or pus, less likely biliverdin from an older bleed.
Peculiar odor: Infection. Listeria may smell sweet, others will be malodorous.
Cord:
VELAMENTOUS INSERTION is a cord attached to the membrane but away from the placenta.
It occurs in maybe 1% of placentas and supposedly places the child at greater risk.
SPONTANEOUS ABORTION
About half of miscarriages supposedly have a chromosomal
abnormality. You'll go crazy trying to sort out what's known (and
what's not) about the other causes, which include "failure to implant"
(nobody knows how common this is), disappearance of the corpus luteum
"because of other endocrine disease", "incompetent cervix",
low folic acid/B6 (i.e., poor diet -- does this run with some other
lifestyle-related risk factor? JAMA 288: 1867, 2002; Ob. Gyn.
100: 107, 2002),
and of course antiphospholipid antibody and
(especially later in the course of the pregnancy) congenitally
hypercoagulable blood (NEJM 343: 1015, 2000; Ann. Int. Med. 130:
736, 1999; Factor V-Leiden is now infamous and generally the thrombophilias are
well-established causes of loss of pregnancies -- "prothrombin G20210A" is
evidently an exception Ob. Gyn. 115: 14, 2010). Contrary
to older ideas, nowadays
assisted reproductive
technology probably isn't a risk for loss later in pregnancy (Ob. Gyn. 114: 818, 2009).
If the amniotic sac ruptures early in pregnancy (perhaps from amniotic band syndrome),
an astute pathologist can spot vernix (desquamated cells from the baby)
in granulomas in the lost tissue.
BLIGHTED OVUM / ANEMBRYONIC PREGNANCY features a good placenta and
membranes but no baby (due to a known or unknown genetic defect --
some of these are triploid and this fades into moles). It is common and now easily
recognized on ultrasound; often this is a sad surprise for a
woman who think she has a normal pregnancy.
The pathologist will eventually see the villi; unlike hydatidiform mole,
there's atrophy rather than proliferation of
trophoblast, and the edema of the villi
isn't impressive.
You
already know that donated
ova have a higher rate of miscarriage (about a third) even if the ovum
is known to have implanted.
Previous elective abortion (either surgical or by the increasingly-popular
methods involving taking medication) do not seem to place a woman at risk
for future miscarriage or ectopic pregnancy (NEJM 357: 648, 2007).
Today there is some interest in bacterial vaginosis
and chlamydia as causes of loss of the unborn child
before viability (Am. J. Ob. Gyn. 183: 431, 2000; others).
After a miscarriage, curettage of the endometrium
yields necrotic tissue, often intensely inflamed with neutrophils.
There will of course always be decidua, and often villi if they
have not been passed.
* Lancet 371: 290, 2008 reports that 68,000 women
die yearly from unsafe abortions in countries where the procedure
is illegal. Obviously, this is an estimate, and I don't understand
how it was reached.
FETAL DEATH
No one really knows how often problems with the cord cause the child's death,
but it must be fairly common.
Often the dead child remains in the amniotic fluid for days or weeks, and
pathologists can estimate the time since death of these "macerated" babies.
(The unborn child is in a sterile environment and thus autolyzes rather than putrefies.)
A "papyraceus" fetus is a twin who died and whose body was flattened
by the other child's.
ECTOPIC PREGNANCY (Am. Fam. Phys. 72: 1707, 2005)
The usual location is the oviduct, though ovary, peritoneum,
and uterine cornua are other known sites. Rarely an intraperitoneal pregnancy
goes to term. The best-known cause is old pelvic inflammatory disease, less often
scarring from endometriosis. But about
half of cases in the US happen "for no reason." In countries
where there is much more gonorrhea, there are many more ectopic pregnancies.
No matter where the pregnancy is, the local cells decidualize and
the child develops for a while. In a tubal pregnancy, disaster
strikes at about 6 weeks after the
missed period (about 8 weeks after conception). One of the following
happens:
Treatment is surgical. Or if an ectopic pregnancy is known to be present
but has not ruptured, methotrexate can end it.
PROBLEMS IN LATE PREGNANCY
Many of the problems that develop toward the end are
caused by problems with the umbilical cord. Of course, if the cord
is compressed enough to occlude the veins, the child is in grave
danger. This includes slip knots, cord around neck, or cord being
compressed by the child's head against the cervix.
Infections can pass through a ruptured membrane
and produce
inflammation of the amnion (amnionitis) and cord (funisitis).
Common bacteria (a pathologist can spot fusobaterium using a silver stain)
can infect the placenta (villitis, chorioamnionitis), as can syphilis ABRUPTION OF THE PLACENTA is a huge bleed between the placenta
and the wall. It is among the most dreaded obstetrical complications.
PLACENTA PREVIA occurs when the placenta covers the lower
uterine segment over the cervical
outlet. This can cause premature labor by affecting the
placenta. As the cervix dilates, bleeding occurs.
{15876} abruption of the placenta, sectioned in situ
You remember the mnemonic for the infections of the unborn child:
* Pathologists are just now starting to examine placenta
changes in children with cerebral palsy, and the results are not
very surprising: clots, partial abruption, inflammation, widespread
infarction (Arch. Path. Lab. Med. 124: 1785, 2000).
* Fun to know: Cesarean section means "to cut". It has nothing to do
with Julius Caesar or laws that he passed. Even in ancient times,
it was routine to take the child by C-section when it was obvious the
mother would die.
* The old rule was, "Once a cesarean, always a cesarean."
In the early 1990's, politics for some reason dictated that
"every women deserves a trial of vaginal delivery no matter how many
cesarean sections she's had previously". This became a "cause for women's advocates"
who distributed "informational literature",
and then became a mandate by practice groups and third-party payers.
And as any reasonable person would expect,
it led to a great many catastrophic deaths (uterine rupture,
placenta accreta, amniotic fluid embolization). For an account
of the fiasco, see ACOG Practice Bulletin 104: 203, July 2004.
Today, the practice recmmendation is that as long as there's been only
one cesarean section, and
it was with a low-transverse incision (or maybe a lower-segment vertical incision),
and resuscitation is available in case of disaster,
the woman
should be given a CHOICE of a trial of vaginal delivery. DON'T
try vaginal delivery if there was a classical incision used for the cesarean section.
TWINS
Think about it.
One chorion, two amnions: A membrane separates the children, but
it contains only an amniotic layer, not a chorionic layer.
They must be monozygotic twins. Okay, there was one reported exception:
NEJM 349: 154, 2003 (in vitro fertilization, donor oocytes).
Two chorions: A membrane or two separates the children, and contains
both chorion and amnion. They
may be monozygotic or dizygotic (fraternal) twins. Dichorionic
placentas can be separate or fused.
The major hazard is a one-way channel between the twins' umbilical cords.
This causes twin-twin transfusion syndrome. The twin who gets the blood
will be big and can die of circulatory overload. The twin who loses the blood
will be small and can die of anemia. Repairing it in-utero: Am. J. Ob. Gyn. 198:
e4, 2008.
An "acardius" is a very malformed fetus with no heart. It can survive if
it is anastomosed to a normal twin.
TOXEMIA OF PREGNANCY (Am. Fam. Phys. 70: 2317, 2004)
Somewhere in the world, a women dies every three minutes from
causes related to toxemia of pregnancy (Curr. Op. OB-Gyn, 14: 119, 2002).
Long a major mystery of medicine, the mystery of toxemia of pregnancy
is just now being clarified.
The key molecule is sFlt1 (now "soluble vascular
endothelial growth factor receptor-1, sVEGFR-1), a tyrosine kinase that
binds to VEGF and other factors. This ends up having
a variety of actions on blood vessels, including inhibiting their
growth and causing
them to leak (J. Clin. Inv. 111: 600, 649, & 707, 2003;
NEJM 350: 672, 2004; Hypertension 55: 689, 2010). Ordinarily, this is the "brakes" on
vascular proliferation late in pregnancy. In toxemia of pregnancy,
it appears too soon.
The process begins when the placenta becomes ischemic.
Poor trophoblastic invasion, insufficiency of the uterine arteries, or
goodness-knows-what sets it up.
Once begun, a vicious cycle starts. Something (evidently sFlt1)
is released by the
ischemic placenta that causes endothelial swelling (raising blood
pressure) and leakage (proteinuria and edema),
and damage sufficient to produce DIC. All of this is
pre-eclampsia.
When the woman has had a seizure, it's "eclampsia" and the mother and
baby are both at grave risk.
Further, lethal disease in one twin is likely to cause pre-eclampsia
that can be cured by destroying the affected twin to permit safe
continuation of the remaining twin's gestation to term (Am. J. Ob. Gyn. 191:
477, 2004).
* Perhaps the reason that it occurs most often in the first pregnancy
is the finding (awaiting confirmation) that women who have had very little
(<4 months) exposure to semen are at much greater risk (Am. J. Ob. Gyn. 188: 1241, 2003).
Can you think of why this makes sense? Remember that half of the placental antigens
are contributed by Dad. If you are not prudish, see
J. Repro. Imm. 46: 155, 2000 for a correlation between
a popular practice between husband and wife and how it seems to protect from pre-eclampsia.
Pre-eclampsia is considered non-preventable, but restricting
sodium, resting, and maybe prescribing antihypertensive medications can stave off eclampsia.
Don't worry about "the usual suspects" produced
by the ischemic placenta -- thromboxanes,
angiotensin, endothelium, and so forth.
The morphology is distinctive.
Update on the histopathology: The clincial correlation with the pathology is so-so (Am. J. Ob. Gyn. 194: 1050, 2006).
Delivery is curative.
When there is also hemolysis, elevated liver enzymes, and low platelet
count (findings that typically run together), we make the additional diagnosis
of HELLP SYNDROME.
I've predicted that the
placenta produces some toxic factor that remains to be discovered;
there is now a report that it is CD95, the fas ligand (Gastroent. 126:
849, 2004) and/or endothelin-1 (J. Clin. Endo. Metab. 90: 4205, 2005).
There are more players as well, and the process
is obviously a complex mix of problems (Am. J. Ob. Gyn. 194: 317, 2006).
ACUTE FATTY LIVER OF PREGNANCY
HYDATIDIFORM MOLE
About one pregnancy in 1000 in the US is a mole. It's much more common
in China and Southeast Asia.
A hydatidiform mole looks like a mass of grapes, as each villus
swells up. The pathologist will see villi with very poor or absent
blood vessels (i.e., mostly just myxoid stuff; after all, there is no
fetal heart to perfuse the chorionic vessels)
and a lot of edema. The amount of trophoblast on the surfaces
is variable and probably means nothing.
"Partial" moles (twice as common as classic moles)
have unevenly swollen villi, trophoblastic
proliferation is minimal, they may have a non-viable baby
with them, and they are 69,XXY or 69,XXX. The extra set
can come from either parent.
The two lesions can't always be distinguished histologically.
A triploid mole is much less likely than a diploid mole to
go on gestational
trophoblastic disease (Cancer 100: 1411, 2004).
Update on the clinical features: BJOG 114: 1273, 2007.
* You can be
a good doctor without knowing the karyotypes of hydatidiform moles, but
it's a triumph of science and a favorite trivia question.
Future truly hardcore pathologists: You can tell a partial mole from a complete mole
because the former stains with a p57 that is only expressed from
the maternal chromosomes (Am. J. Surg. Path. 25: 1225, 2001).
Usually the uterus is larger than it should be,
and bleeding and loss occurs in the fifth month. If the serum hCG levels
have been monitored, they are higher than normal.
Once delivered, the only risk is that an invasive mole
or choriocarcinoma may develop. This will be announced by
persistent elevations of hCG after the mole is gone.
Around 10% of complete moles
go on to cause gestational trophoblastic disease (i.e., invasive mole
or choriocarcinoma), but only about 1% of
partial moles.
Grossly, the tumor is mushy and ultra-bloody (since trophoblast by its
nature invades blood vessels). The tumor has always disseminated widely
by the time it is diagnosed.
Microscopically, there will be no villi. The pathologist will see cytotrophoblast
and syncytiotrophoblast, usually in alternating layers.
Formerly, this was uniformly lethal. Today, the large majority are cured with chemotherapy.
* There are several other lesions involving gestational trophoblast.
Leave their diagnosis to us.
"Exaggerated placental site" is a non-problem.
"Syncytial endometritis" / "placental site nodule"
calls for serial hCG measurements but usually causes no trouble.
"Placental site trophoblastic tumor" is composed of variant
trophoblastic cells and produce human placental lactogen (and maybe
don't produce hCG).
It usually follows a normal birth, lacks the
anaplasia of a real choriocarcinoma, and produces
a distinctive glomerular lesion with fibrin and IgM in the loops
(Ob. Gyn. 114:
465, 2009)
Some choriocarcinomas take the forms of other
familiar carcinomas, especially squamous.
* Acupuncture and other "alternative" medicines (with the exception of black cohosh and
phytoestrogens) completely fail for relief of menopausal syndromes (Ann. Int. Med. 137:
805, 2002).
One does not have to be any kind of militant to be concened with "women's issues", both
nationally and on a global scale. The facts are appalling. Today, the brave
resistance illustrated in Goya's famous picture is being re-enacted with some success.
We can hope for a better tomorrow, but in the meantime, we can help make the changes.
For more on violence,
estrogen replacement, the bendictin fiasco,
female genital mutilation, the pap smear faisco,
fetal monitoring, emergency contraception,
trafficking, and forced marriage, see the online version
of these notes.
Physicians are natural leaders in helping us look for solutions,
and in setting good examples.
![]() Chorangioma
Chorangioma
WebPath Case of the Week
If you, the clinician, do a delivery, the standard of care is to
do and record a sixty-second examination of the placenta. This will
also protect you if things don't go well with mother and/or child.
A few hospitals send all placentas to the pathology lab. More often,
the physician will decide.
General: At term, weighs about a pound (weights variously given at 350-600 gm or so),
abot an inch thick (2.0-2.5 cm), 9-10 inches (15-25 or so cm) across.
Smells like placenta, strongest on fetal side (you'll learn.)
Thin placenta: Think of intrauterine growth retardation from placental insufficiency.
Maternal surface: Deep maroon. Looks complete, no cotyledons absent.
If there's something
missing, it's still inside Mom and the "retained placental tissue" will bleed and/or
get infected.
Fetal surface: Membranes are gray, glistening, and translucent, showing the maroon villi through them.
The broken membrane edges don't bear any large vessels; if they do, there
may well be an extra lobe still inside Mom.
* Meconium itself does not produce inflammation.
It means the child has had a bowel movement, usually from being in distress.
If this happened a while ago, there will be a foreign body reaction
around the meconium. Remember that the child may also have inhaled meconium
("meconium aspiration").
Usually 55-60 cm, 2.0-2.5 cm across. Less than 40 cm or more than
70 cm send to pathologist. There may be true knots,
or an artery may twist and make a false knot. A very twisted cord can supposedly
compromise blood flow, but most babies with "telephone cord cords" seem fine. Check the number of vessels (two arteries and a vein)
near the baby, since the artieries often fuse near the placenta.
Around 1 known pregnancy in 6 ends with miscarriage (i.e., loss of the child
before 20 weeks). The true number
of lost conceptions is
undoubtedly higher as they are very early (i.e., "the period is late").
Loss of the child in the second trimester is uncommon;
as with earlier loss, finding the cause is seldom easy (Am. Fam. Phys. 76: 1341, 2007).
However, it's now fairly clear that just as in preterm birth,
histologic chorioamnionitis, bacterial infection, and viruses
are important causes (Am. J. Ob. Gyn. 195: 797, 2006) --
and of course "intimate partner violence" (Lancet 373: 278, 2009).
We have already talked about problems with the baby (hydrops fetalis,
infections) that can be lethal. Disease of the placenta can obviously
be fatal or damaging as well.
This occurs whenever the embryo implants someplace other
than the normal intrauterine location. (Contrary to some textbooks,
you're not a officially a fetus until you're eight weeks.)
Old cesarean scars are also noteworthy
as sites for ectopic pregnancies (BJOG 113: 1035, 2006).
In the liver: Ob. Gyn. 109: 544, 2007.
The pathologist can help make the diagnosis in a woman
who may be bleeding, by finding decidualized endometrial tissue with
no villi.
{00102} tubal pregnancy, gross
{40140} ectopic pregnancy, gross
{40365} ectopic pregnancy, gross
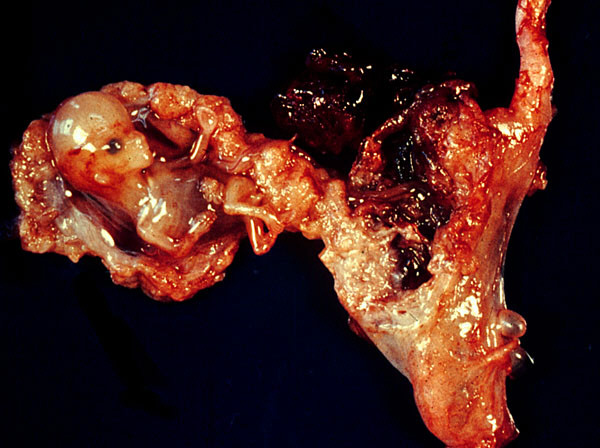
![]() Ruptured Ectopic Pregnancy
Ruptured Ectopic Pregnancy
Text and photomicrographs. Nice.
Human Pathology Digital Image Gallery
![]() 9 week fetus
9 week fetus
Ectopic pregnancy
Wikimedia Commons
* Click here
for the bizarre way in which ectopic pregnancies must be handled in El Salvador, where it is illegal
to end the life of an unborn child EVEN to save the mother's life and
even though the child's chances of being born are zero.
You will learn about the problems in advanced pregnancy while you
are on "OB".
These are among the causes of "late decelerations" and so forth
observed on fetal monitoring. If you, the child, are
not getting enough oxygenated blood after
a contraction has been going on for a while, your heart may slow.
Infections (strep![]() ,
gonorrhea, listeria, others) can involve
the membranes, causing them to rupture early. Sexual intercourse
late in pregnancy can promote these infections. Or a leak may
"just happen", producing oligohydramnios sequence and/or fetal loss
depending on the timing.
,
gonorrhea, listeria, others) can involve
the membranes, causing them to rupture early. Sexual intercourse
late in pregnancy can promote these infections. Or a leak may
"just happen", producing oligohydramnios sequence and/or fetal loss
depending on the timing.
![]() ,
toxoplasmosis
,
toxoplasmosis![]() ,
and TB
,
and TB![]() . If you see granulomas, think of listeria.
A chlamydia infection is likely to produce red eyes in the newborn.
The one established fungal culprit is candida (look for classic "thrush" on the
umbilical cord). In malaria
zones, involvement of placenta often permanently damages the baby (Hum. Path. 32: 1022, 2001).
Thankfully there's
not much brucellosis in the US any more.
. If you see granulomas, think of listeria.
A chlamydia infection is likely to produce red eyes in the newborn.
The one established fungal culprit is candida (look for classic "thrush" on the
umbilical cord). In malaria
zones, involvement of placenta often permanently damages the baby (Hum. Path. 32: 1022, 2001).
Thankfully there's
not much brucellosis in the US any more.
PLACENTA ACCRETA is a portion of placenta that lacks decidua,
adhering instead directly to the myometrium. This is mostly a problem
because after birth, the placenta will separate only with
difficulty and there will be bleeding. One known cause is an
old cesarean scar.
PLACENTA INCRETA is deep into the myometrium. PLACENA PERCRETA is through the myometrium.
![]() Placenta accreta
Placenta accreta
WebPath
T: Toxoplasmosis
![]()
O: Other (syphilis![]() ,
TB
,
TB![]() , listeria)
, listeria)
R: Rubella![]()
C: Cytomegalovirus![]()
H: Herpes simplex II![]()
![]() Rubella of the placenta
Rubella of the placenta
Advanced students
Yutaka Tsutsumi MD
One chorion, one amnion: No membrane separates the children.
They must be monozygotic (identical) twins.
{15651} twin placenta
{39022} twin placenta, gross
{39989} monochorionic monoamniotic twin
{15709} in utero death of a twin
![]() Stillborn twin
Stillborn twin
* This seems pretty well established; a United Nations
panel has accepted it as the best direction for further study:
Ob. Gyn. 109: 168, 2007).
Risk factors include hydatidiform mole, twins, diabetes, obesity, malnutrition
(selenium deficiency? Am. J. Ob. Gyn. 189: 1343, 2003),
high blood
pressure, kidney disease, and the thrombophilias (for the last, see Am. J. Ob. Gyn. 200: 46.e1, 2009).
Newly-recognized is (maybe!) vitamin D deficiency (J. Clin. Endo. Metab. 92:
3517, 2007). Most often it happens during the first
pregnancy.
The placenta &/or unborn child's physiology
probably contributes something, since if Dad is the product
of a pregnancy with pre-eclampsia, the risk is double (NEJM 355: 867, 2001).
* A Dutch group that does a lot of sampling of chorionic villi
has reported that first-trimester pregnancies where the vessels
are close to the intervillous space are more likely to go onto
toxemia (Am. J. Ob. Gyn. 202: 88e, 2010).
This dread, thankfully rare illness seems to be caused by carrying
a child with recessively-inherited mitochondrial disease of fat metabolism
(JAMA 288: 2163, 2002), also possibly etiologic in HELLP syndrome.
This is the most common of the diseases of trophoblast of pregnancy
("gestational
trophoblastic disease").
"Complete" or "classic" moles have no associated baby, and the
villi are uniformly swollen.
The surrounding trophoblast is hyperplastic, growing in sheets.
They have all the chromosomes from
the father ("diandrogenetic"; "daddy's girl"), and are 46XX (usually, two sperms or a duplicated
set from one sperm) or (much less often) 46XY (two sperms).
{27062} hydatidiform mole, histology
{08921} hydatidiform mole, histology
{08922} hydatidiform mole, histology
{18785} hydatidiform mole
INVASIVE MOLE ("chorioadenoma destruens")
This is hypertrophic
trophoblast with at least some villi, penetrating deep into, and maybe through,
the uterine wall, following a hydatidiform mole.
Villi may embolize but not metastasize (i.e., they won't grow into tumors at remote sites).
This lesion is benign and will regress, and is now easily cured
by chemotherapy. The major danger is uterine hemorrhage while the disease
is active.
CHORIOCARCINOMA
This is vicious cancer of the trophoblast. The greatest risk is following
a hydatidiform mole, but any pregnancy (term, ectopic, miscarriage, abortion)
can rarely give rise to "chorio".
{25185} choriocarcinoma, gross (looks like ketchup)
{49378} choriocarcinoma with right ovary, gross
{49379} choriocarcinoma, gross
{25186} choriocarcinoma, histology
{25187} choriocarcinoma, histology
{27056} choriocarcinoma, uterus, histology
{27059} choriocarcinoma, uterus, histology
{40660} choriocarcinoma, histology
 Choriocarcinoma
Choriocarcinoma
Classic drawing
Adami & McCrae, 1914
![]() Choriocarcinoma
Choriocarcinoma
WebPath
![]() Choriocarcinoma
Choriocarcinoma
Tom Demark's Site
![]() {47859} pregnant
{47859} pregnant

 Ectopic pregnancy
Ectopic pregnancy